How a Whole-Food, Plant-Based Diet Can Boost Your Health
There’s excellent scientific evidence that many chronic diseases can be controlled, reduced, or even reversed by moving to a whole-food, plant-based diet. Scientific research highlighted in the landmark book The China Study shows that a plant-based diet can reduce the risk of Type 2 diabetes, heart disease, certain types of cancer, and other major illnesses. Many people also report bigger fitness payoffs, more energy, reduced inflammation, and better health outcomes after making the switch.
What is a Whole-Food, Plant-Based Diet?
A whole-food, plant-based diet is based on the following principles:
Whole food describes natural foods that are not heavily processed. That means whole, unrefined, or minimally refined ingredients. Plant-based means food that comes from plants and doesn’t include animal ingredients such as meat, milk, eggs, or honey.
A whole-food, plant-based diet lets you meet your nutritional needs by focusing on natural, minimally-processed plant foods. They may be missing Vitamin B12 and Omega 3 fatty acids and need for supplementing may need to to be considered
Below is a quick overview of the major food categories you’ll enjoy on a plant-based diet, with examples. For a more detailed breakdown of what to eat on a WFPB diet, check out The Forks Over Knives Diet Explained.
Fruits: Any type of fruit including apple, bananas, grapes, strawberries, citrus fruits, etc.
Vegetables: Plenty of veggies including peppers, corn, lettuce, spinach, kale, peas, collards, etc.
Tubers: Starchy root vegetables like potatoes, sweet potatoes, yams, and cassava (aka yuca).
Whole grains: Grains, cereals, and other starches in whole form, such as quinoa, brown rice, whole wheat, oats, popcorn, etc.
Legumes: Beans of any kind, plus lentils, pulses, etc.
There are plenty of other foods you can also enjoy, including nuts, seeds, avocados, tofu, tempeh, whole-grain flours and breads, and plant-based milks. However, we recommend eating these foods in moderation, because they are more calorie-dense and can contribute to weight gain.
THE BENEFITS OF A WHOLE-FOOD, PLANT-BASED DIET
There are several major benefits to moving to plant-based nutrition, all supported by science. Plant-based diet benefits include:
Easy weight management: People who eat a plant-based diet tend to be leaner than those who don’t, and the diet makes it easy to lose weight and keep it off—without counting calories.
Disease prevention: Whole-food, plant-based eating can prevent, halt, and in some cases reverse chronic diseases. The scientific evidence is especially overwhelming when it comes to heart disease and diabetes, but research has also linked plant-based diets to lower rates of arthritis, improved liver function, and healthier kidneys.
A lighter environmental footprint: A plant-based diet places much less stress on the environment.
EASY WEIGHT MANAGEMENT
If you’re looking to lose weight (and keep it off), a whole-food, plant-based diet is one of the most powerful tools at your disposal. Research shows that people who eat plant-based diets tend to be leaner than those who don’t. A 2020 review looked at 19 intervention studies—i.e., studies in which participants were assigned a diet for a specified period of time—and found that in each one, participants assigned to plant-based diets lost weight.
Why are healthy plant-based diets so effective for weight loss? Research suggests that the crux is calorie density. Dairy products and highly processed foods are high in calories yet low in the fiber that helps us feel full and fuels a healthy gut microbiome. Whole plant foods are low in calories, meaning you can eat a high volume of food without exceeding your calorie needs. That’s why on a whole-food, plant-based diet, you’re encouraged to eat until you’re satisfied—no calorie counting or portion control necessary.
A whole-food, plant-based diet is extremely effective at promoting cardiovascular health and preventing, halting, and in some cases even reversing heart disease, the leading cause of death in the United States. A 2019 review of 99 studies found that diets rich in whole plant foods were associated with significantly lower risk of cardiovascular disease compared with diets high in meat and dairy products.
There are several reasons for this. Animal-based foods are high in saturated fat and cholesterol, which raise blood cholesterol levels, causing fatty, wax-like plaque to build up in the arteries. Highly processed foods often contain excessive salt, which raises blood pressure, damaging the lining of the arteries over time. By eliminating these harmful foods from your diet and replacing them with whole plant foods, you can bring down your cholesterol levels, blood pressure, and risk of heart disease. Learn more about diet and heart disease here.
A 2018 report in BMJ Open Diabetes Research & Care found that for people with Type 2 diabetes, plant-based diets were more beneficial than the diets recommended by several diabetes associations, offering greater improvements in physical and emotional well-being.
Plant-based diets are low in saturated fat (a culprit behind insulin resistance) and high in fiber, which helps the body to regulate blood sugar and properly absorb nutrients. Plant-based diets also reduce the risk of being overweight or obese, a primary risk factor for Type 2 diabetes. Learn more about diabetes and diet here.
H
IT’S BETTER FOR THE PLANET
Plant-based diet benefits also extend beyond your own body—switching to a WFPB lifestyle is one of the best things you can do for the environment.
The main reason is that raising animals for food is an incredibly inefficient use of resources. Growing crops to feed animals “introduces a major extra step of waste relative to the efficiency of us just eating the plant foods directly,” explains David L. Katz, MD, MPH, FACPM, FACP, FACLM. “If you just eat the plants, you cut out the middleman.” A 2018 analysis found that livestock provides just 18 percent of calories consumed globally but takes up 83 percent of farmland. Vegan and plant-based, whole-food diets are also associated with fewer climate-altering greenhouse gas emissions.
Whole plant foods are not only the healthiest and most sustainable foods around; they’re also some of the most affordable. In fact, going plant-based can cut grocery bills by $750 a year per person, according to research published in the Journal of Hunger & Environmental Nutrition.
When you stock your kitchen with WFPB staples such as brown rice, potatoes, and dried beans, you can assemble nutritious, satisfying meals for just a few dollars. To showcase just how affordable plant-based diets can be, we’ve put together a budget-friendly one-week vegan meal plan: How to Eat Plant-Based for Just $7 a Day.
While some people like to dive in headfirst and go 100-percent whole-food, plant-based overnight, we know that a sudden lifestyle shift isn’t for everyone. We asked one of our expert contributors, Craig McDougall, MD, for his advice for those who prefer a more gradual approach: “Add around 1,000 calories of legumes, whole grains, and starchy vegetables to your everyday routine. These starchy foods keep you full and satisfied, so you’ll naturally eat less of the animal products and processed foods that are making you sick.” Dr. McDougall has plenty of other great advice to share.
Forks Over Knives founder Brian Wendel has some good tipstoo. He encourages people to “not sweat the small stuff” and to look at the big picture instead: “Focus on the big changes like switching from meat, milk, and eggs to whole plant foods. Such changes dramatically improve the nutritional composition of your diet, so this is where you will find the most noticeable and measurable improvements in your health.”
Whether you go all-in or decide to make a gradual shift, the time to start making the change is now. You’ll be glad you did.
FREE DOWNLOAD
7 Keys To Success on a Healthy Diet
Getting started on a plant-based diet or looking to refresh your eating habits? Download our practical guide to long-term success.
LET US MAKE WHOLE-FOOD, PLANT-BASED LIVING EASIER
We’ve worked with leading chefs, nutritionists, and developers to create a variety of tools that make it easy for you to adopt and maintain a healthy plant-based lifestyle.
Meal Planner
Forks Meal Planner takes the work out of deciding what to eat. Each week you’ll get a customized meal plan, plus a dynamic grocery list and a time-saving weekend prep guide.
Learn to cook whole-food plant-based like a pro with our online cooking course.You’ll master everything from proper knife skills to oil-free cooking and seasoning.
Recipe App
Filled with hundreds of recipes, our top-rated recipe app can help you out of a cooking rut and keep you from falling into one ever again.
Books & Magazines
With stunning food photography, helpful how-tos, and tips from plant-based experts, our collection of cookbooks and magazines has everything you need.
USEFUL RESOURCES AND READING
Forks Over Knives Helpful Articles
YOUR PLANT-BASED QUESTIONS, ANSWERED
We’re sure you’ve got questions about the move to a whole-food, plant-based diet, and we’re here to help.
How do I eat out on a plant-based diet?Most restaurants are very accommodating of dietary needs, and you should be able to review their menu online. Scan the menu in advance to see if a restaurant offers vegan options, and you’re already most of the way there. When you’re unsure, simply call ahead, explain your preferences, and they will probably be able to accommodate you.
How do I make sure I get the nutrients I need?Whole plant foods contain all the essential nutrients (with the exception of vitamin B12) we need. You can get some B12 from fortified foods such as plant-based milks and breakfast cereals, but the best source is a simple B12 supplement. (In fact, the U.S. Department of Health and Human Services recommends supplemental B12 for all adults over age 50 because as we age, many people lose the ability to absorb vitamin B12 from food sources.)READ MOREHow to Order a Healthy Plant-Based Meal from Any Restaurant Menu
Is a whole-food, plant-based diet the same as being vegan?While there are certainly some similarities between eating a whole-food, plant-based diet and being vegan, there are some key differences as well.Vegans avoid all animal products or exploitation in food, clothing, shoes, or any other aspect of their lives. Vegans do not necessarily focus on whole plant foods; they may eat refined and processed foods, although many choose not to. By comparison, a whole-food, plant-based diet is defined as one that eliminates or minimizes all animal products and highly refined foods, including oil. Loading up on fiber-rich, nutrient-dense, close-to-nature foods makes it simple to meet your nutritional needs without exceeding your caloric needs. FOK teaches the gold standard plant-based diet, which is completely free of animal products and therefore vegan.
New Zealand: Green kiwifruit or psyllium consumption could be a suitable dietary treatment for relieving constipation and associated gastrointestinal (GI) comfort, states a recent study published in The American Journal of Gastroenterology.
“Our study provides original evidence that the consumption of fresh, whole fruit can increase the frequency of bowel movements in constipated people,” Richard Gearry from the University of Otago, Christchurch, New Zealand, and colleagues wrote in their study. ” Also, there was a significant improvement in stool consistency, reduction in indigestion, constipation, and abdominal pain leading to an improved overall level of GI comfort.”
Patients are increasingly looking for evidence-based natural treatments for many medical conditions, including constipation. Many patients believe natural products are less costly and safer than prescription medications. Owing to this, so-called ‘functional foods’ are increasing in popularity.
Previous studies have shown that consuming green kiwifruit relieves constipation. Also, there were reported improvements in gastrointestinal comfort. The researchers’ team, therefore, investigated the effect of green kiwifruit consumption on GI function and comfort.
The study included 63 healthy controls (HC), 61 patients with constipation-predominant irritable bowel syndrome (IBS-C) and 60 with functional constipation (FC). They were randomly assigned to daily consumption of two green kiwifruits (7.5 g) followed by a 4-week wash-out, and then the other treatment ensued for four weeks.
The number of CSBM (complete spontaneous bowel movements) per week was determined (primary outcome). Secondary outcomes of GI comfort included the gastrointestinal symptom rating scale (GSRS). Intent-to-treat (ITT) data was analyzed as a difference from baseline through repeated measures analysis of variance appropriate for AB/BA cross-over design.
The study led to the following findings:
· Green kiwifruit consumption was linked with a clinically relevant increase of ≥ 1.5 CSBM per week (FC; 1.53, IBS-C; 1.73) and remarkably improved measures of GI comfort (GSRS total score) in constipated people (FC, IBS-C).
· No significant adverse events were observed.
Findings from the international multicenter controlled trial of kiwifruit as a constipation treatment provide evidence that consuming a fresh, whole fruit has shown clinically relevant increases in complete spontaneous bowel movements and improved GI comfort in constipated people.
“Green kiwifruit is a suitable dietary treatment for relieving constipation and associated GI comfort,” the authors concluded.
Reference:
Gearry, Richard MD, PhD*,a,1; Fukudo, Shin MD, PhD*,2,7; Barbara, Giovanni MD*,3; Kuhn-Sherlock, Barbara PhD4; Ansell, Juliet PhD5; Blatchford, Paul PhD5; Eady, Sarah6; Wallace, Alison PhD6; Butts, Christine PhD6; Cremon, Cesare MD3; Barbaro, Maria Raffaella PhD3; Pagano, Isabella MD3; Okawa, Yohei PhD2; Muratubaki, Tomohiko PhD2; Okamoto, Tomoko PhD8; Fuda, Mikiko9; Endo, Yuka MD7; Kano, Michiko MD, PhD2; Kanazawa, Motoyori MD, PhD2,7; Nakaya, Naoki PhD10; Nakaya, Kumi PhD10; Drummond, Lynley B. Tech (Hons.)11. Consumption of two green kiwifruit daily improves constipation and abdominal comfort – results of an international multicentre randomized controlled trial. The American Journal of Gastroenterology ():10.14309/ajg.0000000000002124, December 20, 2022. | DOI: 10.14309/ajg.0000000000002124
Infertility, or failure to achieve clinical pregnancy after 1 year of unprotected intercourse, affects up to 15% of couples worldwide. Estimated US prevalence of women with impaired fertility has increased from 4.5 million in the early 1980s to ~7.7 million by 2025.
Most women with infertility have reproductive or neuroendocrine disorders, such as premature ovarian insufficiency, oligomenorrhea or amenorrhea, anovulation, poor gamete quality, and other reproductive diseases. Mechanisms of women’s infertility may include genetic factors and exposure to reproductive toxicants, such as heavy metals increasingly released into the environment by industrial development, agricultural practices, and production and use of consumer products.
Study Synopsis and Perspective
Background
Infertility in women has been attributed to both genetic factors and exposure to reproductive toxicants.
Cadmium, lead, and mercury are 3 primary heavy metals listed by the World Health Organization (WHO) as being among the top 10 toxicants of major public health concern.
Women’s reproductive health is vulnerable to environmental toxins, particularly endocrine-disrupting chemicals that interfere with the body’s normal hormone synthesis, secretion, and signaling.
Growing epidemiological and experimental evidence links heavy metals to endocrine-disrupting properties, suggesting a possible causal relationship with women’s infertility and other reproductive disorders.
Most previous studies have had small sample sizes and have focused on a single metal.
Study Design
Data were analyzed for women of reproductive age who participated in the 2013 to 2018 National Health and Nutrition Examination Survey (NHANES) and had blood heavy metals data, including 1999 patients for the comparison of ever-infertile (238 patients) versus fertile (1761 patients) patients and 297 patients for the comparison of ever-infertile (238 patients) versus pregnant (59 patients) patients.
Multiple logistic regression models were used to examine the associations.
Key Results
there was a positive association between lead concentrations and women’s ever-infertility: As blood lead concentrations increased, women were more likely to be ever-infertile (odds ratio [OR], 1.75) versus fertile and ever-infertile (OR, 3.09) versus pregnant.
No differences were seen for cadmium and mercury concentrations.
For the analysis of ever-infertile versus pregnant patients, blood concentrations of lead in quartiles 3 and 4 were significantly associated with women’s historical infertility (OR, 3.47 and 5.26, respectively), with a dose-dependent relationship seen from quartiles 2 to 4.
Disclosures
Study Highlights
Using NHANES 2013 to 2018, 1999 women were identified for analysis of infertility (238 ever-infertile; 1761 fertile) and 1,919 for analysis of long-term amenorrhea.
Percentages of women who exceeded typical or normal levels of blood heavy metals were 18.5% for lead, 0.05% for cadmium, and 0.9% for mercury.
Blood concentrations of lead and heavy metal mixtures were significantly higher in ever-infertile women than pregnant women, but concentrations of cadmium and mercury were similar.
There was a significant and dose-dependent positive association between blood lead concentrations and women’s historical infertility, a negative association between cadmium and long-term amenorrhea, and no associations between mercury and heavy metal mixture and women’s infertility
As blood lead concentrations increased, women were more likely to be ever-infertile than fertile (OR, 1.75) or pregnant (OR, 3.09).
For analysis of ever-infertile vs pregnant, lead blood concentrations in quartiles 3 and 4 were significantly associated with women’s historical infertility
The investigators concluded that significant percentages of women had blood heavy metal levels exceeding typical or normal levels, that blood concentrations of single lead and heavy metal mixtures were associated with increased historical infertility,
Female reproductive health is vulnerable to environmental toxins, particularly heavy metals and other endocrine-disrupting chemicals interfering with normal hormone synthesis, secretion, and signaling.
Overall, the risk for heavy metal exposure to women’s reproductive health and fertility mandates prevention and reduction of heavy metal exposure, which is an urgent, unmet need.
Genetic factors and reproductive toxicant exposure may both contribute to female infertility.
WHO’s top-10 list of toxicants of major public health concern includes cadmium, lead, and mercury.
As animal studies found that cadmium may adversely affect female reproduction, the finding that cadmium was protective against long-term amenorrhea was unanticipated.
Future research is needed to evaluate associations among cadmium levels, dietary patterns, iron levels, and amenorrhea.
Experimental research suggests that lead may affect female fertility via various mechanisms, including menstrual cycle disruption, altered hormone levels, and impaired fetal development.
In mouse models, lead accumulates in the ovary and disrupts folliculogenesis, reduces ovarian reserve, and increases follicle atresia, all of which may contribute to lead-induced historical infertility.
Evidence is insufficient to draw meaningful conclusions about how mercury affects female reproductive outcomes, highlighting the need for additional research.
Clinical Implications
Exposure to heavy metals had differential associations with women’s infertility and long-term amenorrhea.
Overall, the risk for heavy metal exposure to women’s reproductive health and fertility mandates prevention and reduction of heavy metal exposure, which is an urgent, unmet need.
Implications for the Health Care Team: Members of the healthcare team should educate women of childbearing age about the risks posed by exposure to heavy metals, including cadmium, lead and mercury.
The study covered in this summary was published in medRxiv as a preprint and has not yet been peer reviewed.[1]
Study funding: National Institutes of Health (NIH).
Author disclosures: NIH, one author received start-up funds from the Environmental and Occupational Health Sciences Institute at Rutgers University.
Severe Hypertension + Drinking Two Or More Cups Of Coffee Per Day = Increases The Risk Of Cardiac Deaths
Numerous studies have been conducted on the advantages of coffee consumption, however if a person has high blood pressure, they may want to limit their intake to one cup per day. A heart attack, stroke, or other cardiovascular illness might increase the chance of death for those with hypertension who consume two or more cups of coffee each day, according to a study that was published in the American Heart Association’s peer-reviewed journal. However, green tea or one cup of coffee a day didn’t have the same impact.
In this new research, we see drinking two or more cups of coffee per day may double the risk of death from cardiovascular disease in individuals with severe high blood pressure (160/100 mm Hg or higher) but not in individuals with high BP that is not considered severe. In contrast, even though both beverages contain caffeine, the study revealed that one cup of coffee and daily a cup of green tea drinking did not raise the risk of death from cardiovascular disease at any blood pressure measurement. An 8-ounce cup of green or black tea contains 30-50 milligrams of caffeine, whereas an 8-ounce cup contains more than 80 to 100 mg.
What effect does caffeine have on blood pressure?
Even if we do not have high blood pressure, caffeine can induce a brief but substantial increase in blood pressure. It is unknown what causes this increase in blood pressure. Caffeine’s effect on blood pressure varies from one person to another. According to some research, caffeine may interfere with a hormone that keeps the arteries open. Others believe that coffee stimulates the adrenal glands to produce more adrenaline, which raises blood pressure. Some people who drink caffeinated beverages on a regular basis have a higher average blood pressure than those who do not. Others who consume caffeinated beverages on a regular basis adhere to a caffeine tolerance. Caffeine has no long-term effect on blood pressure a result.
Previous research has shown that drinking one cup of coffee per day can benefit heart attack survivors by lowering their risk of death after a heart attack and can help prevent heart attacks or strokes in healthy persons. According to another study, drinking coffee on a regular basis may lower the risk of developing chronic illnesses such as Type 2 diabetes and some cancers; may help to control appetite; may help to lower the risk of depression or boost alertness, though it is unclear whether this effect is due to caffeine or something else in coffee. On the negative side, excessive coffee consumption can result in high blood pressure, anxiety, heart palpitations, and difficulty in sleeping. The study’s goal, according to senior author Hiroyasu Iso, M.D., Ph.D., M.P.H., director of the Institute for Global Health Policy Research, Bureau of International Health Cooperation, National Center for Global Health and Medicine in Tokyo, Japan, and professor emeritus, is to determine whether coffee’s known protective effect also applies to individuals with varying degrees of hypertension. As far as we are aware, this is the first study to show a connection between daily coffee intake of two or more cups and mortality from cardiovascular disease in those with severe hypertension.
High blood pressure, often known as hypertension, occurs when the volume of blood pressing against the blood vessel walls is consistently too high, causing the heart to work harder to pump blood. Mercury millimetres are used to measure it (mm Hg). According to the American Heart Association and the American College of Cardiology’s most recent blood pressure recommendations, hypertension is defined as a value of 130/80 mm Hg or greater. The study’s blood pressure requirements varied somewhat from the ACC/AHA recommendations.
the ideal and normal blood pressure range is less than 130/85 mm hg;
high normal is between 130 and 139/85- and 89 mm hg;
grade 1 hypertension is between 140 and 159/90- and 99 mm hg;
grade 2 hypertension is between 160 and 179/100- and 109-mm hg;
and grade 3 hypertension is greater than 180/110 mm hg.
blood pressure levels in grades 2 and 3 were severe hypertension in this investigation. more than 12,000 women and over 6,570 men, aged 40 to 79 at the commencement of the study, participated in it. they were chosen from the japan collaborative cohort study for evaluation of cancer risk, a sizable prospective study of individuals residing in 45 japanese municipalities that were conducted between 1988 and 1990. through health exams and self-administered questionnaires examining lifestyle, food, and medical history, participants gave data. through 2009, after almost 19 years of follow-up, 842 cardiovascular-related fatalities were recorded. data analysis for all participants revealed the following:
People with blood pressures of 160/100 mm Hg or above were twice as likely to die from cardiovascular disease as those who did not drink two or more cups of coffee each day. No research it was proved that blood pressure increased by having a daily cup of coffee and was not related to a higher risk of dying from cardiovascular disease.
Across all blood pressure groups, drinking green tea was not linked to an increased risk of cardiovascular disease death.
The conclusion that patients with severe high blood pressure should refrain from excessive coffee consumption may be supported by these data, according to Iso. Caffeine’s adverse effects may outweigh its preventive properties and may raise the risk of mortality because those with severe hypertension are more vulnerable to its aftermath. Regardless of the blood pressure group, individuals who drank coffee more regularly were younger, current drinkers and smokers, ate fewer vegetables, had higher total cholesterol levels and had lower systolic blood pressure (top number). The inclusion of polyphenols, which are micronutrients found in plants that have beneficial antioxidant and anti-inflammatory properties, may assist to explain the benefits of green tea.
The effects of green tea on blood pressure
There are several dietary supplements on the market, but the evidence supporting their usefulness is inconsistent. One of the most loved beverages of all is green tea. Green tea extracts are known to be antioxidants and ACE inhibitors. Green tea polyphenols also prevent lipid absorption from the intestines and aid in the conversion of cholesterol to bile acids. Epidemiologic research has revealed that green tea has a cardioprotective impact, and evidence synthesis has revealed that green tea intake relates to blood vessel relaxation. We assessed and consolidated information from clinical studies investigating the effect of green tea on blood pressure and lipid profile to evaluate the effect of green tea intake on blood pressure and lipid profile. A daily intake of 5-6 cups of green tea may result in lower systolic blood pressure, total cholesterol, and LDL cholesterol. Green tea should not be used as a replacement for the present treatment of people with hypertension or dyslipidemia. Green tea looks to be well tolerated; however excessive drinking may result in unpleasant consequences. Because the effects of long-term green tea consumption are unknown, longer-term independent clinical investigations are required.
Even though both green tea and coffee contain caffeine, the researchers are of the opinion that polyphenols may play a role in why only coffee intake related to an elevated risk of mortality in those with severe high blood pressure. There are numerous drawbacks to the study: Coffee and tea consumption were self-reported; blood pressure was measured at a single point, which did not account for changes over time; and due to the study’s observational nature, a direct cause-and-effect relationship between coffee consumption and cardiovascular disease risk among people with severe high blood pressure could not be drawn. The impacts of coffee and green tea intake in patients with high blood pressure and the consequences of coffee and green tea consumption in other nations both require additional research, according to the experts.
What traditional Indian medicine teaches about eating well with diabetes
August 02, 2022
Susan Weiner, MS, RDN, CDCES, FADCES, talks with Parul Kharod,MS, RD, LDN, about the ancient medical knowledge system known as Ayurveda and what it can reveal about living with diabetes.
Weiner:What is Ayurveda and how does it apply to Indian cuisine?
The ancient medical knowledge system Ayurveda teaches that all disease begins in the gut and that food is medicine, and traditional foods cooked with ayurvedic principles tend to be healthy.
Kharod: Ayurveda is an ancient medical system dating back more than 5,000 years. Ayur means “life,” and veda means “knowledge.” Thus, Ayurveda is the knowledge of how to live a healthy, happy life. According to Ayurveda, health is not absence of disease. Ayurveda focuses on preservation of a healthy body and prevention of disease. The principles of Ayurveda focus on each person’s unique constitution and aim to bring balance of mind, body and spirit in a personalized approach.
The principal tenet of Ayurveda is that all disease begins in the gut — and it’s likely Hippocrates learned that from Ayurveda. According to Ayurveda, all diseases occur due to dysfunction of agni, the digestive fire that helps with metabolism and digestion of food, maintains the natural gut flora by killing foreign bacteria and toxins, and supports the growth of healthy bacteria.
Ayurveda categorizes three doshas as substances that flow or circulate within the body, bringing disease through excess or deficiency. The doshas exhibit the characteristics of the elements from which they are made. All diseases are caused by an imbalance of the doshas, and imbalance is caused by intake of improper diet and by leading an unhealthy lifestyle.
Food itself is the medicine. Our physical makeup is a combination of five essential elements present in the universe: ether, air, fire, water and earth. According to Ayurveda, six tastes originate from these five elements: sweet, sour, salty, pungent, bitter and astringent. We need each of these six tastes in our daily diet. Indian cuisine is richly flavored with these six tastes to aid in optimal digestion.
Ayurveda also categorizes foods as heating or cooling to the body. There are norms about combinations of foods and what foods should or should not be eaten at the same meal. Dietary goals change with the seasons and according to stages of the lifecycle. The aim is restoring the balance of natural energies; digesting food well; building strong cells and tissues, including our immune cells; having regular and complete elimination; keeping sharp senses; achieving peace of mind; and maintaining clear thinking.
Weiner:What are your top culinary tips for people who live with diabetes when eating traditional Indian food?
Kharod: Traditional foods cooked with ayurvedic principles tend to be healthy and easy to digest. However, not everyone eats that way. Indian food can also be unhealthy, especially when prepared with excess oils and heavy creams. If meals are not properly balanced, they can be high in simple starches.
I use the plate method to talk about portion control. My first tip is to increase the amount and variety of non-starchy vegetables. Second, swap simple starches and flour for intact whole grains. I encourage use of plant-based proteins, such as legumes, nuts and seeds. Another tip is to reduce salt, sugar and fat in the diet.
Weiner:What should someone consider when adopting a plant-based diet?
Kharod:There is a huge misconception that vegetarians only eat vegetables. People trying to adopt a plant-based diet may either consume inadequate calories and nutrients, if they are eating only salads, or they may get excess calories, if they are eating veggie burgers and mock chicken nuggets. A plant-based diet should always revolve around plants. Eating real foods that grow as plants — whole grains, beans and lentils, nuts, seeds, fruits and vegetables. Limit packaged processed foods, especially imitation meats. It is important to eat balanced meals that are colorful and dense in nutrients.
Weiner:How can a person with diabetes reduce carbohydrate consumption while eating traditional Indian foods?
Kharod: Eating for diabetes is not only about reducing carbohydrates, but about reducing sugars and simple starches. Research shows that a high-fat diet may also have a negative effect on insulin resistance. Timing of meals, spacing of meals and balance of the plate are also important. It is important to focus on fiber rather than just carbohydrates. Foods that are rich in healthy carbohydrates and fibers include all intact whole grains, beans, peas and lentils. Traditional recipes using flours can be modified to use intact whole grains. I give out recipes and information on how traditional foods can be modified and made lower in carbohydrate and higher in fiber.
Weiner: What are some tips for incorporating spices into meals?
Kharod: Spices are incorrectly confused with the term “spicy,” meaning hot. This is not true. Only varieties of peppers are hot. Most other spices have unique tastes. Indian food cannot be cooked without spices. In fact, all foods should be cooked with spices and herbs, as these are not just for flavor. All spices have healing anti-inflammatory properties, and are composed of an impressive list of phytonutrients, essential oils, antioxidants, minerals and vitamins that are vital for good health.
Get familiar with variety of spices and start using them. Add cinnamon, cardamom and nutmeg to oatmeal and even coffee. Add turmeric and ginger to soups and stir fries. Use cumin-flavored black beans in your tacos. As you start using them, you will feel more comfortable to experiment. In the meantime, rely on recipes.
Weiner: Where can people with diabetes learn more about Indian cuisine?
Kharod: Physicians should refer their patients to a registered dietitian specializing in Indian cuisine and/or plant-based diets who can consider the person’s overall health and prescribe an individualized nutrition plan. Information on consumer websites may not be accurate or may make recommendations for people with diabetes without considering comorbid heart disease or kidney disease.
For more information:
Parul Kharod, MS, RD, LDN, is a registered dietitian and licensed nutritionist practicing in Raleigh/Cary, North Carolina. She can be reached atparulkharod@gmail.com.
Susan Weiner, MS, RDN, CDN, CDCES, FADCES, is co-author of The Complete Diabetes Organizer and Diabetes: 365 Tips for Living Well. She is the owner of Susan Weiner Nutrition PLLC and is the Endocrine Today Diabetes in Real Life column editor. She can be reached at susan@susanweinernutrition.com; Twitter: @susangweiner.
This information is for general information only and may not apply to you. Also it gets out of date as medicine progresses. Please check with your provider prior to any action or concern. You must remember it is in general positive results are dealing with probabilities of getting the disease and if positive may adversely affect you mentally causing anxiety and depression
Genes contain information about how you look and how your body works; they are passed from parents to children (inherited).
Genetic testing looks for abnormalities (also called ” harmful( pathogenic) variants, alterations, or mutations) in certain genes. The result of genetic testing can help you understand your risk for developing certain diseases, such as breast, ovarian, prostate, or pancreatic cancer. Testing for pathogenic variants in several different genes is available.
Pathogenic variants have different implications, depending on whether they are carried in the “germline” (inherited from a parent or happening during early embryonic development) or “acquired” (arising at any time in a person’s life e.g exposure to radiation)
In hereditary cancer syndromes, the pathogenic variant is present in the germline, meaning it is present in an egg or sperm cell and passed from parent to child at the time of conception. If a person inherits a germline variant, it is usually present in every cell in their body. This means that the person may be at risk for several types of tumors over their lifetime.
They may benefit from increased monitoring to detect cancer at an earlier and more treatable stage and/or interventions such as prophylactic (preventive) surgery to lower the risk of developing cancer.
If you have inherited a germline pathogenic variant, it also means that you could pass it on to your children. This differs from cancers in which genetic variants found in the tumor cannot be passed on to children. However, some families may have a high risk of breast or ovarian cancer caused by a gene variant that has not yet been identified, and increased monitoring or other interventions may be appropriate in family members without cancer. In every situation a consultation with a hereditary cancer or cancer genetics expert is essential.
Between 5 and 10 percent of breast cancers and up to 20 percent of ovarian cancers are caused by germline variants. Approximately 10 to 15 percent of pancreatic and metastatic prostate cancers are due to genetic causes. The genes most often involved are known as BRCA1 and BRCA2.
Genetic testing for hereditary breast, ovarian, pancreatic, and prostate cancers includes analysis of the BRCA1 and BRCA2 genes for pathogenic variants.
There is also “next-generation” multigene or panel testing, which includes analysis of a number of genes in which variants are associated with hereditary cancer. For example, panels may assess only those genes in which variants are associated with very high risks of certain cancers. Larger panels may also include more moderate-risk genes or newer genes, for which less information is known about cancer risks and the management recommendations may be less clear. Genetic testing is done on a sample of saliva or blood.
WHO SHOULD CONSIDER GENETIC TESTING?
Your health care provider can help you understand your personal and family history and whether you might be a candidate for genetic counseling and testing. Ultimately, the decision is up to you.
Commonly used guidelines — In general, experts typically recommend genetic counseling and consideration of BRCA1/2 testing if you have (or have had):
●A personal history of breast cancer that falls into any of the following categories:
•Diagnosed at age 50 or younger, or 60 or younger for “triple-negative” breast cancer (a type of breast cancer that lacks proteins on the surface of its cells called estrogen and progesterone hormone receptors and human epidermal growth factor 2 [HER2] receptors [ie, ER, PR, and HER2 negative]).
•Cancer in both breasts (either at the same time or at separate times), with the first one diagnosed at age 50 or younger.
•Male breast cancer.
•Diagnosed at any age, in addition to having one or more close relatives with breast cancer at age 50 or younger or ovarian, male breast, metastatic prostate, or pancreatic cancer at any age.
●A personal history of ovarian, pancreatic, or metastatic prostate cancer.
●A personal and/or family history (on the same side of the family) of three or more of certain types of cancer (including, but not limited to, breast, colon, and pancreatic cancer).
●No personal history, but first- or second-degree relatives with breast cancer diagnosed at age 50 or younger, ovarian cancer, male breast cancer, pancreatic cancer, or metastatic prostate cancer.
●Ashkenazi Jewish ancestry (from Central or Eastern Europe), regardless of personal or family history, but especially if there is a personal history of breast, ovarian, pancreatic, or metastatic prostate cancer.
●One or more biological relatives who have tested positive for a pathogenic variant in BRCA1 or BRCA2, or other genes associated with hereditary cancer.
There are other situations in which genetic counseling and/or testing may also be recommended. An individualized risk assessment can help you determine whether genetic testing might be useful for you. Your health care provider can assess your personal risk; there are different tools and mathematical models they can use for this.
If you have not had cancer and are concerned about hereditary risk (for example, if you have had multiple relatives with breast or ovarian cancer), the usual recommendation is to offer testing first to someone in the family who has had cancer, if possible.
Usually this means testing a woman with ovarian cancer or breast cancer who was diagnosed at the youngest age within the family. If that person is found not to have a harmful variant, it may not be helpful to test family members without cancer.
Some companies sell at-home testing kits (these are also called “direct-to-consumer” tests). Usually the kits involve paying a fee and mailing in a sample of your saliva to a lab for testing. While some of these companies test only for genes that give information about your ancestry, others have expanded to test for pathogenic variants that can increase your risk of certain cancers, such as BRCA1 and BRCA2. However, these tests may not be comprehensive as they may only look at a small subset of the possible pathogenic variants in these genes, and/or they may not look at other genes that are also associated with hereditary cancers. In addition, if you choose to take one of these at-home tests and get a positive result, it’s important that you submit another sample to a clinical lab for confirmation.
If you are interested in this type of testing, you should discuss this with your health care provider or a genetic counselor first. They can help make sure you understand your results as well as the limitations of these tests.
GENETIC TESTING PROCESS
Pretest counseling — Before you have genetic testing, it is important to speak with a genetics or health care provider to better understand your level of risk for cancer. This involves a discussion of your personal and family history in order to better understand your risk for getting cancer in the future. The provider may also use mathematical models or calculators to help estimate your risk and discuss the following:
●Your options for genetic testing
●The risks, benefits, and limitations of testing
●The potential outcomes of the recommended test(s)
●The potential impact of your test results on family members
If you are interested in talking with a genetic counselor or genetics service provider, your health care provider can help you find one in your area.
Costs and insurance coverage — Genetic testing is offered by many different labs. The cost can vary widely depending on the extent of testing that is performed.
Many people worry about how the results of genetic testing will affect the chance of getting health or life insurance in the future. In the United States, a federal law known as the Genetic Information Nondiscrimination Act (GINA) prohibits health insurers and most employers with 15 or more employees from using your genetic information to discriminate against you. This law is intended to encourage Americans to take advantage of genetic testing if needed. In general, the law means that:
●Most employers cannot deny you a job or fire you because of the results of genetic testing.
●Health insurers cannot use genetic testing results to deny you coverage or set your insurance rates.
●Employers and insurers cannot require you to have genetic testing.
It’s important to be aware that the law does not have protections for disability, life insurance, or long-term care insurance. In addition, GINA does not apply to individuals in the military. State laws may provide additional coverage.
INTERPRETING THE RESULTS
It is not always easy to interpret the results of genetic tests. The results may be:
●Positive for a BRCA1 or BRCA2 or other harmful variant – This means that a variant was identified that is known to be associated with increased risks for cancer. It does not mean that you have cancer or will definitely get it.
●Negative, meaning that you do not have a variant in the genes that were tested – This result does not rule out the possibility that you may still have a hereditary risk for cancer. It is possible that your genetic testing did not include all known genes associated with cancer, nor all variants known to be present in the gene(s) tested. In addition, there are unknown genetic variants that have not yet been discovered.
●A “true” negative result – This means that a pathogenic variant that is present in one or more of your family members (for example, your mother, sibling, or aunt) was ruled out in you. This result usually means that your cancer risks are about the same as other people in the general population. However, your health care provider or genetic counselor will assess your other risk factors for cancer.
●Positive for a variant of “unknown significance” (VUS) – This means that you have a genetic change or variant, but it is not clear whether it increases your risk of cancer; it is possible to have a variant that does not affect cancer risk. Over time, most VUS results are reclassified as positive or negative. More often than not, most VUS results are reclassified as negative. It is important to keep in contact with your health care provider to ensure that you will receive updated information if this happens.
It’s important to keep in mind that a negative result does not mean that you will not develop cancer, and a positive result does not mean that you will definitely develop cancer.
The following is information specific to pathogenic variants in the BRCA1/2 genes. For information about other genes associated with hereditary breast and ovarian cancer, talk with your genetic counselor or health care provider.
For people who test positive for a BRCA1/2 pathogenic variant, the lifetime risk of developing certain types of cancer is estimated as follows:
●Female breast cancer – The lifetime risk (to age 70) of breast cancer is between 55 and 70 percent for BRCA1 and 45 to 70 percent for BRCA2. This means that in a group of 100 women with BRCA1, between 55 and 70 of the women will develop breast cancer in their lifetime. Some women may develop more than one breast cancer over the course of their lifetimes, sometimes on the opposite side compared to where their first breast cancer developed (in such cases, called “contralateral breast cancer”).
●Ovarian cancer – The lifetime risk of ovarian cancer is about 40 percent for BRCA1 and 15 percent for BRCA2.
●Male breast cancer – The lifetime risk of male breast cancer is about 1 percent for BRCA1 and 8 percent for BRCA2.
●Pancreatic cancer – The lifetime risk of pancreatic cancer is about 2 to 4 percent for BRCA1 and 5 percent for BRCA2.
●Prostate cancer – The lifetime risk of pancreatic cancer is about 15 to 20 percent for BRCA1 and 30 to 40 percent for BRCA2.
POST-TEST COUNSELING
After genetic testing is done, it is important to talk to your health care provider or genetics provider to make sure you understand what the results mean for you and your family. During this discussion you can find out how your test results affect your cancer risk and what options are available to you to detect cancer early or reduce your risk. Your health care provider or genetic counselor will answer your questions as well as provide resources for more information and support.
If you test positive for a pathogenic variant in a gene such as BRCA1 or BRCA2, it is important that you talk with your family about the results. Family members may want to talk to their own provider and/or obtain genetic counseling to discuss the option of genetic testing.
MANAGING THE RISK OF CANCER
If you test positive for a BRCA1/2 pathogenic variant, there are several ways to screen for cancer and to reduce your risk of developing cancer.
For women, you may
●Have more frequent screening for breast and ovarian cancer
●Have surgery to reduce your risk of breast and/or ovarian cancer
●Take a medicine to reduce your risk of breast or ovarian cancer
For men, you may have more frequent prostate cancer screening.
The best strategy might include a combination of these methods. It is important to understand that the aim of screening is to detect a cancer at its earliest stage, when it is most likely to be curable. The aim of prevention (or risk-reducing strategies) is to reduce the risk of ever developing cancer.
If you test negative for a BRCA1/2 pathogenic variant but have a family history of breast or ovarian cancer, talk to your health care provider about ways to manage your risk of developing cancer.
Screening options
Breast cancer screening — Increased screening is recommended for both women and men with a BRCA1/2 pathogenic variant.
Women who have a BRCA1/2 pathogenic variant are usually advised to have:
●A breast exam, performed by a health care provider, every 6 to 12 months beginning at age 25
●A mammogram once per year, beginning at age 30 (or possibly earlier, depending on family history)
●A breast magnetic resonance imaging (MRI) once per year, beginning at age 25 (or possibly earlier, depending on family history)
●”Breast awareness,” beginning at age 18, which involves paying attention to changes in the breasts and may include regular breast self-exams
Men who have a BRCA1/2 pathogenic variant are usually advised to have:
●Monthly breast self-examinations, beginning at age 35, in order to be aware of any changes in the breasts
●A breast exam, performed by a health care provider, every 12 months beginning at age 35
Men are not routinely advised to get mammograms for screening, although it may be considered in certain situations.
Ovarian cancer screening — In general, screening tests for ovarian cancer are not very accurate in detecting the disease. However, screening may be an option for some women who have a BRCA1/2 variant. This involves a combination of a blood test (called “CA 125”) and a pelvic ultrasound. Some experts recommend this combination of tests every six months, beginning at age 30 (or earlier, if the woman had a relative who was diagnosed with ovarian cancer before 30).
Prostate cancer screening — Men with a BRCA2 pathogenic variant should begin prostate cancer screening at age 40. Men with a BRCA1 pathogenic variant might also consider beginning screening at age 40; other factors, such as the age at diagnosis of any family members who had cancer, may influence the recommendation
Risk-reducing options
Surgery — An alternative to frequent cancer screening is surgery to reduce your risk of developing cancer. This is called preventive (or prophylactic) surgery, and it can significantly decrease your risk of cancer and may help decrease anxiety. Your health care provider can talk to you in detail about the potential risks and benefits of each type of preventive surgery.
The following may be options for reducing cancer risk in women with a BRCA1/2 pathogenic variant; there are no proven risk-reducing surgical options for men.
Mastectomy — Women who have both breasts removed (called “prophylactic bilateral mastectomy”) reduce their chance of developing breast cancer by at least 90 percent. There is a small chance of developing cancer in the residual breast tissue that remains after surgery.
Women who already have breast cancer may also choose to have one or both breasts removed to reduce their risk of developing a second breast cancer. More information about mastectomy, and options for breast reconstruction, is available separately.
Removal of the ovaries — Having the ovaries and fallopian tubes removed (termed a “prophylactic bilateral salpingo-oophorectomy,” or BSO) has been shown to reduce a woman’s risk of ovarian and fallopian tube cancer by 80 to 90 percent, and in premenopausal BRCA2 carriers, it may reduce the risk of breast cancer by 50 to 60 percent.
Women with a BRCA1/2 pathogenic variant are strongly recommended to have a BSO, typically between ages 35 and 40 years (for BRCA1) and 40 and 45 (BRCA2) and once they are done having children.
Medicines to reduce the risk of cancer — There is some evidence that certain medications can reduce the risk of cancer in women in particular situations:
●Medicines such as selective estrogen receptor modulators (eg, tamoxifen) or aromatase inhibitors have been shown to reduce the risk of breast cancer in women who are at increased risk not due to genetic reasons. Based on limited studies, it is possible that these medications are also effective in BRCA2 carriers, but it is unclear if they are in BRCA1 carriers. (
●Hormonal birth control (pill, skin patch, vaginal ring, shot, progestin intrauterine device [IUD], or implant) can decrease the risk of ovarian cancer. Data suggest that this is also true for women with a BRCA1/2 pathogenic variant.
However, it is possible that hormonal birth control may increase the risk of breast cancer, particularly in women who have a BRCA1 pathogenic variant and start birth control at a young age and before their first pregnancy. If you have a BRCA1/2 pathogenic variant, talk to your health care provider about the risks and benefits of hormonal birth control.
You’re probably aware that your body burns energy all the time, no matter what you’re doing.
One way to calculate your body’s energy expenditure is with metabolic equivalents, also known as METs. You might see METs listed on exercise equipment or mentioned by personal trainers to help you measure your physical activity. MET
One metabolic equivalent (MET) is defined as the amount of oxygen consumed while sitting at rest and is equal to 3.5 ml O2 per kg body weight x min. The MET concept represents a simple, practical, and easily understood procedure for expressing the energy cost of physical activities as a multiple of the resting metabolic rate. The energy cost of an activity can be determined by dividing the relative oxygen cost of the activity (ml O2/kg/min) x by 3.5.
A MET is a ratio of your working metabolic rate relative to your resting metabolic rate. Metabolic rate is the rate of energy expended per unit of time. It’s one way to describe the intensity of an exercise or activity.
One MET is the energy you spend sitting at rest — your resting or basal metabolic rate. So, an activity with a MET value of 4 means you’re exerting four times the energy than you would if you were sitting still.
To put it in perspective, a brisk walk at 3 or 4 miles per hour has a value of 4 METs. Jumping rope, which is a more vigorous activity, has a MET value of 12.3.
SUMMARY
METs = metabolic equivalents.
One MET is defined as the energy you use when you’re resting or sitting still.
An activity that has a value of 4 METs means you’re exerting four times the energy than you would if you were sitting still.
To better understand METs, it’s helpful to know a little about how your body uses energy.
The cells in your muscles use oxygen to help create the energy needed to move your muscles. One MET is approximately 3.5 milliliters of oxygen consumed per kilogram (kg) of body weight per minute.
So, for example, if you weigh 160 pounds (72.5 kg), you consume about 254 milliliters of oxygen per minute while you’re at rest (72.5 kg x 3.5 mL).
Energy expenditure may differ from person to person based on several factors, including your age and fitness level. For example, a young athlete who exercises daily won’t need to expend the same amount of energy during a brisk walk as an older, sedentary person.
For most healthy adults, MET values can be helpful in planning an exercise regimen, or at least gauging how much you’re getting out of your workout routine.
Researchers who have monitored oxygen consumption in the muscles of people performing various activities have been able to assign MET values to those activities. These values are based on a person weighing 70 kgTrusted Source, or 154 lbs.
This chart provides approximate MET values for a variety of light, moderate, and vigorous activities.
METs
MET stands for the metabolic equivalent of task. One MET is the amount of energy used while sitting quietly. Physical activities may be rated using METs to indicate their intensity. For example, reading may use about 1.3 METs while running may use 8-9 METs.
METs can also be translated into light, moderate, and vigorous intensities of exercise.
Sedentary—Uses 1.5 or fewer METs. Examples are sitting, reclining, or lying down.
Light intensity—Uses from 1.6-3.0 METs. Examples are walking at a leisurely pace or standing in line at the store.
Moderate intensity—Uses from 3.0-6.0 METs. Examples are walking briskly vacuuming, or raking leaves.
Vigorous intensity—Uses from 6.0+ METs. Examples are walking very quickly, running, taking an aerobics class, or shoveling snow
How you reach those goals — whether it’s through running, hiking, weight training, or any other activity — is less important than simply striving for those targets.
Although just moving more and sitting less offers health benefits, how much energy you use while exercising can increase those health benefits further. This is referred to as energy intensity.
Borg Scale
The Borg Scale of Perceived Exertion measures your exercise intensity by rating how you feel. It is based on observations like higher heart rate, heavier and faster breathing, increased sweating, and muscles feeling tired. It does not use actual measurements of these occurrences but a personal self-check.
The scale uses numbers from 6 to 20. The lowest rating is “no feeling of exertion,” at number 6, and the highest rating is “very, very hard,” at number 20. Moderate activities register 11 to 14 (“fairly light” to “somewhat hard”) while vigorous activities usually rate 15 or higher (“hard” to “very, very hard”). Dr. Gunnar Borg, who created the scale, set it to run from 6 to 20 as a simple way to estimate heart rate—multiplying the Borg score by 10 gives an approximate heart rate for a particular level of activity. [1]The Borg Scale of Perceived Exertion
How you might describe your exertion
Borg rating of your exertion
Examples (for most adults <65 years old)
None
6
Reading a book, watching television
Very, very light
7 to 8
Tying shoes
Very light
9 to 10
Chores like folding clothes that seem to take little effort
Fairly light
11 to 12
Walking through the grocery store or other activities that require some effort but not enough to speed up your breathing
Somewhat hard
13 to 14
Brisk walking or other activities that require moderate effort and speed your heart rate and breathing but don’t make you out of breath
Hard
15 to 16
Bicycling, swimming, or other activities that take vigorous effort and get the heart pounding and make breathing very fast
Very hard
17 to 18
The highest level of activity you can sustain
Very, very hard
19 to 20
A finishing kick in a race or other burst of activity that you can’t maintain for long
Exercise workouts may vary in intensity throughout the session. You can use the Borg Scale to change the intensity, by speeding up or slowing down movements or applying more or less resistance (such as increasing the incline on a treadmill or turning the resistance control knob on a stationary bicycle).
Target Heart Rate
Calculating your heart rate and target heart rate can be used to measure exercise intensity. First determine your maximum heart rate: subtract your age from 220 (example: the maximum heart rate for a 40-year-old person would be 220 – 40 = 180 beats per minute). The target heart rate for moderate-intensity exercise is between 65-75% of your maximum heart rate (or 77-93% of maximum heart rate for vigorous exercise). So for the 40-year-old person with a maximum heart rate of 180, the target heart rate falls somewhere between 117-135 beats per minute for moderate exercise, or 139-167 for vigorous exercise.
Then measure your actual heart rate in either of these two ways:
Midway through the exercise, stop to check your pulse. Place the tips of your index and middle fingers at the wrist and press lightly on the artery in line with the thumb. Count the heartbeats for 30 seconds and multiply by 2.
Wear a heart rate monitor. Some pedometers have a built-in heart rate monitor that displays your current heartbeats per minute.
The current guidelines from the American Heart Association (AHA) focus on dietary interventions to reduce the risk for cardiovascular disease, and other chronic illnesses.
Mediterranean-style diet is associated with a lower risk for type 2 diabetes.
In addition, the Dietary Approaches to Stop Hypertension (DASH) diet has been associated with a slower decline in age-associated cognitive tasks, and the Mediterranean diet can reduce cognitive decline as well. Finally,
higher consumption of nuts, low-fat dairy products, and legumes, along with moderate alcohol consumption, is associated with a lower risk for severe renal disease.
Higher consumption of artificially sweetened beverages, sugar-sweetened beverages, and red meat is associated with worse renal outcomes.
The current guidelines provide some interesting opinions and facts regarding current dietary trends.
Study Synopsis and Perspective
In a new scientific statement on diet and lifestyle recommendations, the AHA is highlighting, for the first time, structural challenges that impede the adoption of heart-healthy dietary patterns.
This is in addition to stressing aspects of diet that improve cardiovascular health and reduce cardiovascular risk, with an emphasis on dietary patterns and food-based guidance beyond naming individual foods or nutrients.
VERY IMPORTANT STATEMENT: STEP BACK AND LOOK
“The way to make heart-healthy choices every day,” said Dr Lichtenstein, from the Jean Mayer USDA Human Nutrition Research Center on Aging at Tufts University in Boston, in a statement, “is to step back, look at the environment in which you eat, whether it be at home, at work, during social interaction, and then identify what the best choices are. And if there are no good choices, then think about how you can modify your environment so that there are good choices.”
The statement, published in Circulation, underscores growing evidence that nutrition-related chronic diseases have maternal-nutritional origins, and that prevention of pediatric obesity is a key to preserving and prolonging ideal cardiovascular health.[1]
The features are as follows:
Adjust energy intake and expenditure to achieve and maintain a healthy body weight. To counter the shift toward higher energy intake and more sedentary lifestyles over the course of past 3 decades, the statement recommends at least 150 minutes of moderate physical activity per week, adjusted for individual’s age, activity level, sex, and size.
Eat plenty of fruits and vegetables; choose a wide variety. Observational and intervention studies document that dietary patterns rich in varied fruits and vegetables, with the exception of white potatoes, are linked to a lower risk for cardiovascular disease (CVD). Also, whole fruits and vegetables, which more readily provide fiber and satiety, are preferred over juices.
Choose whole grain foods and products made mostly with whole grains rather than refined grains. Evidence from observational, interventional, and clinical studies confirms the benefits of frequent consumption of whole grains over infrequent consumption or over refined grains in terms of CVD risk, coronary heart disease (CHD), stroke, metabolic syndrome, cardiometabolic risk factors, laxation, and gut microbiota.
Choose healthy sources of protein, mostly from plants (legumes and nuts).
Higher intake of legumes, which are rich in protein and fiber, is associated with lower CVD risk, whereas higher nut intake is associated with lower risks for CVD, CHD, and stroke mortality/incidence. Replacing animal-source foods with plant-source whole foods, beyond health benefits, lowers the diet’s carbon footprint. Meat alternatives are often ultraprocessed, and evidence on their short- and long-term health effects is limited. Unsaturated fats are preferred, as are lean, nonprocessed meats.
Use liquid plant oils rather than tropical oils (coconut, palm, and palm kernel), animal fats (butter and lard), and partially hydrogenated fats. Saturated and trans fats (animal and dairy fats, and partially hydrogenated fat) should be replaced with nontropical liquid plant oils. Evidence supports the cardiovascular benefits of dietary unsaturated fats, especially polyunsaturated fats primarily from plant oils (eg, soybean, corn, safflower, and sunflower oils; walnuts; and flax seeds).
Choose minimally processed foods instead of ultraprocessed foods. Because of their proven association with adverse health outcomes, including overweight and obesity, cardiometabolic disorders (type 2 diabetes, CVD), and all-cause mortality, the consumption of many ultraprocessed foods is of concern. Ultraprocessed foods include artificial colors and flavors and preservatives that promote shelf stability, preserve texture, and increase palatability. A general principle is to emphasize unprocessed or minimally processed foods.
Minimize intake of beverages and foods with added sugars. Added sugars (commonly glucose, dextrose, sucrose, corn syrup, honey, maple syrup, and concentrated fruit juice) are tied to elevated risk for type 2 diabetes, high cholesterol, and excess body weight. Findings from meta-analyses on body weight and metabolic outcomes for replacing added sugars with low-energy sweeteners are mixed, and the possibility of reverse causality has been raised.
Choose and prepare foods with little or no salt. In general, the effects of sodium reduction on blood pressure tend to be higher in Black people, middle-aged and older people, and those with hypertension. In the United States, the main combined sources of sodium intake are processed foods, those prepared outside the home, packaged foods, and restaurant foods. Potassium-enriched salts are a promising alternative.
If you don’t drink alcohol, don’t start; if you choose to drink, limit intake.
Although relationships between alcohol intake and cardiovascular outcomes are complex, the 2020 Dietary Guidelines Advisory Committee recently concluded that those who do drink should consume no more than 1 drink per day and should not drink alcohol in binges; the 2020 Dietary Guidelines for Americans continues to recommend no more than 1 drink per day for women and 2 drinks per day for men.
Adhere to the guidance regardless in all settings. Food-based dietary guidance applies to all foods and beverages, regardless of where prepared, procured, and consumed. Policies should be enacted that encourage healthier default options (for example, whole grains, minimized sodium and sugar content).
Recognizing Impediments
The AHA/American Stroke Association (ASA)scientific statement closes with the declaration: “Creating an environment that facilitates, rather than impedes, adherence to heart-healthy dietary patterns among all individuals is a public health imperative.” It points to the National Institutes of Health’s (NIH’s) 2020-2030 Strategic Plan for NIH Nutrition Research,[2] which focuses on precision nutrition as a means “to determine the impact on health of not only what individuals eat, but also of why, when, and how they eat throughout the life course.”[1]
Ultimately, precision nutrition may provide personalized diets for CVD prevention. But the “food environment,” often conditioned by “rampant nutrition misinformation” through local, state, and federal practices and policies, may impede the adoption of heart-healthy dietary patterns. Factors such as “targeted food marketing [for example, of processed food and beverages in minority neighborhoods], structural racism, neighborhood segregation, unhealthy built environments, and food and nutrition insecurity create environments in which unhealthy foods are the default option.”
These factors compound adverse dietary and health effects and underscore a need to “directly combat nutrition misinformation among the public and health care professionals.” They also explain why, despite widespread knowledge of heart-healthy dietary pattern components, little progress has been made in achieving dietary goals in the United States.
Study Highlights
Diet is one of the most important modifiable risk factors for CVD. High adherence to a healthy diet can reduce the risk for cardiovascular mortality by 14% to 28% compared with low adherence.
Energy needs decline with age by an average of 70 to 100 kcal/day for each decade of life. Balancing energy consumption is the first recommendation from the current guidelines.
The consumption of fruits and vegetables is encouraged. Deeply colored fruits and vegetables, such as leafy greens and peaches, tend to be more nutrient-dense vs lighter-colored foods.
The guidelines encourage consumption of all forms of fruits and vegetables: fresh, frozen, canned, and dried. Frozen fruits and vegetables offer similar or higher nutrient content compared with fresh fruits and vegetables, but they have a longer shelf-life and are often less expensive.
The replacement of refined grain with whole grains is associated with a lower risk for coronary heart disease.
Higher consumption of legumes is associated with a reduced risk for CVD. The guidelines cite soybeans, lentils, chickpeas, and split peas as good examples of legumes.
Higher consumption of nuts is associated with lower risks for coronary heart disease as well as a reduced risk for stroke incidence and mortality.
The authors caution against the rush to plant-based meat alternatives as a healthier option. These products are ultraprocessed and contain added sugar, saturated fat, salt, stabilizers, and preservatives. There is little evidence regarding the health effects of meat alternatives at this time.
Two to 3 servings of fish per week is associated with lower risks for all-cause mortality, coronary heart disease, stroke, and heart failure. Replacing foods rich in saturated fat with fish is particularly salutary, although fried fish does not provide the same health benefits.
The authors recommend replacing full-fat dairy products with nonfat and low-fat dairy products, although they acknowledge that the data to support this recommendation are evolving and controversial.
Consumption of red meat should be limited, as should consumption of processed meat. Processed meat has an even stronger positive association with CVD than red meat.
However, the consumption of unprocessed poultry does not appear to significantly affect the risk for CVD.
The consumption of polyunsaturated fats provides a moderate advantage over the consumption of monounsaturated fats in the prevention of CVD.
Added sugars are to be avoided. Meta-analyses of clinical trials have reported mixed outcomes for low-energy sweeteners on body weight and metabolic outcomes.
Low-abundance mono- and disaccharides may provide a healthier option than added sugars, but there are not enough data on these products as yet.
Sodium consumption should be minimized, particularly among Black individuals, middle-aged and older adults, and patients with hypertension. Replacing sodium with potassium is a promising strategy to reduce blood pressure.
Alcohol consumption is associated with higher risks for hemorrhagic stroke and atrial fibrillation. There is a J- or U-shaped relationship between alcohol consumption and coronary heart disease, with the lowest risk apparent among adults who consume 1 or 2 alcoholic beverages per day. The AHA does not support the initiation of alcohol consumption for cardiovascular health.
It is better to obtain essential nutrients from dietary sources vs supplements. There is insufficient evidence to support the routine use of high-dose supplements for cardiovascular health.
Reducing the consumption of saturated fat can reduce the risk for CVD by approximately 30%, which is similar to what might be expected with statin therapy.
The recommendations caution against the use of coconut oil, which raises LDL cholesterol compared with other plant-based oils but has not been demonstrated to have other health benefits.
Clinical Implications
The Mediterranean-style diet is associated with a lower risk for type 2 diabetes and cognitive decline. The DASH diet has also been associated with a slower decline in age-associated cognitive tasks. Finally, higher consumption of nuts, low-fat dairy products, and legumes, along with moderate alcohol consumption, are associated with a lower risk for severe renal disease. Higher consumption of artificially sweetened beverages, sugar-sweetened beverages, and red meat is associated with worse renal outcomes.
The current guidelines do not find enough evidence to recommend plant-based meat alternatives, artificially sweetened beverages, or alcohol consumption for the routine prevention of cardiovascular disease. The recommendations state that although processed meat and red meat are associated with higher risks for cardiovascular disease, unprocessed poultry is not.
Implications for the healthcare team: The healthcare team should use the specific advice from the AHA to help guide patients on their dietary choices.
Recent data suggest that mangos could help improve certain risk factors for chronic disease in patients who are overweight or obese, according to researchers.
In addition, two other trials exploring how diet affects health revealed an association between herbs and spices and improvements in BP and cholesterol.
All three studies were presented during the annual meeting of the American Society for Nutrition, held virtually.
Mangos may lower chronic disease risk
In the first study, Martin Rosas Jr., MS, a research assistant at San Diego State University and a campus food and nutrition intern at the Humane Society, and colleagues examined the potential health benefits of mangos in adults with overweight or obesity.
“Mangos contain many beneficial nutrients and have been shown to have health-promoting properties,” Rosas told Healio Primary Care. “We conducted this study to determine if the addition of fresh mangos as a snack food would modify CVD risk factors compared to another commonly consumed type of snack.”
Rosas and colleagues assigned 27 participants to receive either 100 calories of fresh mangos daily or 100 calories of low-fat cookies daily for 12 weeks. After a 4-week washout period, the participants were then assigned to the other dietary intervention.
Neither intervention significantly changed body weight, body fat percentage, BMI or BP, according to the researchers.
Overall, daily mango consumption did not affect anthropometric measurements or lipid profiles, Rosas said during a presentation. There was a significant increase in aspartate transaminase following mango consumption, but there were no changes in the other liver function enzymes, “suggesting minimal effects on liver health from this study,” Rosas said.
There was also an association between mango consumption and improvements in total antioxidant capacity and C-reactive protein. In addition, Rosas reported “a beneficial effect” of mango consumption on fasting blood glucose, which he said may be due to the mangiferin and fiber in mangos.
Meanwhile, the researchers observed a significant increase in insulin and triglycerides after 12 weeks of low-fat cookie consumption.
“Encouraging fruit and vegetable consumption, especially when replacing refined carbohydrates, can reduce the risk of CVD,” Rosas said in the interview. “Mangos should be considered as a healthy snack choice, containing many nutrients, antioxidants and fiber that may reduce certain CVD risk factors, including reductions in fasting blood glucose.”
Herbs, spices may lower BP
In a separate study, Kristina S. Petersen, PhD, APD, FAHA, an assistant professor of nutritional sciences at Texas Tech University, and colleagues assessed the cardiometabolic effects of adding mixed herbs and spices to a typical American diet.
The study included 71 adults who were at higher risk for cardiometabolic disease. They were assigned to receive each of the following diets for 4 weeks, with a minimum 2-week washout period in between interventions: a low-spice diet (0.5 g for every 2,100 kcal per day), moderate-spice diet (3.3 g for every 2,100 kcal per day) or high-spice diet (6.6 g for every 2,100 kcal per day). The herbs and spices included in the analysis were cinnamon, coriander, ginger, cumin, parsley, black pepper, garlic, turmeric, onion powder, rosemary, paprika, chili powder, cilantro, oregano, basil, red pepper, thyme, bay leaf, cardamom, sesame seeds, sage, poppy seeds, dillweed and allspice.
There were no significant changes in blood glucose or LDL cholesterol after the interventions, Petersen said during a presentation. However, after the moderate-spice diet, total cholesterol was 6.8 mg per dL lower than baseline.
“It is unclear why the effect occurred with the moderate-spice diet, with no effect present for the high-spice diet,” Petersen said. “The lack of a dose-response effect suggests that the spices given did not reduce lipid absorption via inhibition of digestive enzymes, which was the hypothesized mechanism by which spices would reduce total and LDL cholesterol.”
Compared with the low- and moderate-spice diet, the high-spice diet was associated with a significant reduction in mean 24-hour systolic BP, which declined by about 3 mm Hg from baseline.
The researchers observed similar effects with diastolic BP. The high-spice diet was associated with a 1.8 mm Hg reduction in diastolic BP compared with baseline, “and this was statistically different from both the low and moderate diets,” Petersen said.
“In conclusion, this study shows that the addition of 6.6 g per day of herbs and spices to an average American diet improved 24-hour BP after 4 weeks compared to lower doses of herbs and spices in adults at elevated risk for cardiometabolic diseases,” she said. “Further research is needed to determine whether adding herbs and spices to a healthy dietary pattern would elicit greater cardiometabolic health benefits.”Melina B. Jampolis
Melina B. Jampolis, MD, a past president of the National Board of Physician Nutrition Specialists who was not affiliated with the study, said the findings “support the idea of cutting back on salt and replacing it with herbs and spices.”
Cholesterol benefits of spices in type 2 diabetes
For the third study, SepidehAlasvand, a PhD student in nutrition and food science at Clemson University in South Carolina, and colleagues investigated the impact of certain spices on cholesterol in patients with type 2 diabetes.
The researchers analyzed 28 randomized controlled trials, which included 1,049 control participants and 1,035 participants who received spice supplements in capsule form. The spices included ginger (eight studies), turmeric (three studies), curcumin (three studies), cinnamon (11 studies) and curcuminoids (three studies). The trial durations ranged from 1 to 3 months, Alasvand said during a presentation.
In general, Alasvand reported that all spice supplements appeared to improve lipid profiles in patients with type 2 diabetes.
“Therefore, these spices may be a potential source for modern dyslipidemia treatments in individuals with type 2 diabetes,” she said.
The findings support previous research that shows that spices can help patients manage their blood glucose and improve cholesterol, according to Jampolis.
“The wonderful thing about spices is that they can improve the flavor of foods, too, so it’s a win-win,” she said. “Patients are more likely to stick with recommendations that are easy and tasty!”
References:
Alasvand S, et al. A systematic review of the effectiveness of ginger, cinnamon, turmeric, curcumin, and curcuminoids for dyslipidemia associated with diabetes. Presented at: American Society of Nutrition Scientific Sessions and Annual Meeting; June 7-10, 2021 (virtual meeting).
Petersen KS, et al. A culinary dose of herbs and spices improves 24-hour blood pressure in adults at risk for cardiometabolic diseases: A randomized, crossover, controlled-feeding study. Presented at: American Society of Nutrition Scientific Sessions and Annual Meeting; June 7-10, 2021 (virtual meeting).
Rosas M, et al. Effects of fresh mango consumption on blood glucose, insulin, and other cardiovascular disease risk factors in overweight and obese adults. Presented at: American Society of Nutrition Scientific Sessions and Annual Meeting; June 7-10, 2021 (virtual meeting).
ADD TOPIC TO EMAIL ALERTS
Recent data suggest that mangos could help improve certain risk factors for chronic disease in patients who are overweight or obese, according to researchers.
In addition, two other trials exploring how diet affects health revealed an association between herbs and spices and improvements in BP and cholesterol.
All three studies were presented during the annual meeting of the American Society for Nutrition, held virtually.
Mangos may lower chronic disease risk
In the first study, Martin Rosas Jr., MS, a research assistant at San Diego State University and a campus food and nutrition intern at the Humane Society, and colleagues examined the potential health benefits of mangos in adults with overweight or obesity.
“Mangos contain many beneficial nutrients and have been shown to have health-promoting properties,” Rosas told Healio Primary Care. “We conducted this study to determine if the addition of fresh mangos as a snack food would modify CVD risk factors compared to another commonly consumed type of snack.”
Rosas and colleagues assigned 27 participants to receive either 100 calories of fresh mangos daily or 100 calories of low-fat cookies daily for 12 weeks. After a 4-week washout period, the participants were then assigned to the other dietary intervention.
Neither intervention significantly changed body weight, body fat percentage, BMI or BP, according to the researchers.
Overall, daily mango consumption did not affect anthropometric measurements or lipid profiles, Rosas said during a presentation. There was a significant increase in aspartate transaminase following mango consumption, but there were no changes in the other liver function enzymes, “suggesting minimal effects on liver health from this study,” Rosas said.
There was also an association between mango consumption and improvements in total antioxidant capacity and C-reactive protein. In addition, Rosas reported “a beneficial effect” of mango consumption on fasting blood glucose, which he said may be due to the mangiferin and fiber in mangos.
Meanwhile, the researchers observed a significant increase in insulin and triglycerides after 12 weeks of low-fat cookie consumption.
“Encouraging fruit and vegetable consumption, especially when replacing refined carbohydrates, can reduce the risk of CVD,” Rosas said in the interview. “Mangos should be considered as a healthy snack choice, containing many nutrients, antioxidants and fiber that may reduce certain CVD risk factors, including reductions in fasting blood glucose.”
Herbs, spices may lower BP
In a separate study, Kristina S. Petersen, PhD, APD, FAHA, an assistant professor of nutritional sciences at Texas Tech University, and colleagues assessed the cardiometabolic effects of adding mixed herbs and spices to a typical American diet.
The study included 71 adults who were at higher risk for cardiometabolic disease. They were assigned to receive each of the following diets for 4 weeks, with a minimum 2-week washout period in between interventions: a low-spice diet (0.5 g for every 2,100 kcal per day), moderate-spice diet (3.3 g for every 2,100 kcal per day) or high-spice diet (6.6 g for every 2,100 kcal per day). The herbs and spices included in the analysis were cinnamon, coriander, ginger, cumin, parsley, black pepper, garlic, turmeric, onion powder, rosemary, paprika, chili powder, cilantro, oregano, basil, red pepper, thyme, bay leaf, cardamom, sesame seeds, sage, poppy seeds, dillweed and allspice.
There were no significant changes in blood glucose or LDL cholesterol after the interventions, Petersen said during a presentation. However, after the moderate-spice diet, total cholesterol was 6.8 mg per dL lower than baseline.
“It is unclear why the effect occurred with the moderate-spice diet, with no effect present for the high-spice diet,” Petersen said. “The lack of a dose-response effect suggests that the spices given did not reduce lipid absorption via inhibition of digestive enzymes, which was the hypothesized mechanism by which spices would reduce total and LDL cholesterol.”
Compared with the low- and moderate-spice diet, the high-spice diet was associated with a significant reduction in mean 24-hour systolic BP, which declined by about 3 mm Hg from baseline.
The researchers observed similar effects with diastolic BP. The high-spice diet was associated with a 1.8 mm Hg reduction in diastolic BP compared with baseline, “and this was statistically different from both the low and moderate diets,” Petersen said.
“In conclusion, this study shows that the addition of 6.6 g per day of herbs and spices to an average American diet improved 24-hour BP after 4 weeks compared to lower doses of herbs and spices in adults at elevated risk for cardiometabolic diseases,” she said. “Further research is needed to determine whether adding herbs and spices to a healthy dietary pattern would elicit greater cardiometabolic health benefits.”Melina B. Jampolis
Melina B. Jampolis, MD, a past president of the National Board of Physician Nutrition Specialists who was not affiliated with the study, said the findings “support the idea of cutting back on salt and replacing it with herbs and spices.”
Cholesterol benefits of spices in type 2 diabetes
For the third study, SepidehAlasvand, a PhD student in nutrition and food science at Clemson University in South Carolina, and colleagues investigated the impact of certain spices on cholesterol in patients with type 2 diabetes.
The researchers analyzed 28 randomized controlled trials, which included 1,049 control participants and 1,035 participants who received spice supplements in capsule form. The spices included ginger (eight studies), turmeric (three studies), curcumin (three studies), cinnamon (11 studies) and curcuminoids (three studies). The trial durations ranged from 1 to 3 months, Alasvand said during a presentation.
In general, Alasvand reported that all spice supplements appeared to improve lipid profiles in patients with type 2 diabetes.
“Therefore, these spices may be a potential source for modern dyslipidemia treatments in individuals with type 2 diabetes,” she said.
The findings support previous research that shows that spices can help patients manage their blood glucose and improve cholesterol, according to Jampolis.
“The wonderful thing about spices is that they can improve the flavor of foods, too, so it’s a win-win,” she said. “Patients are more likely to stick with recommendations that are easy and tasty!”
References:
Alasvand S, et al. A systematic review of the effectiveness of ginger, cinnamon, turmeric, curcumin, and curcuminoids for dyslipidemia associated with diabetes. Presented at: American Society of Nutrition Scientific Sessions and Annual Meeting; June 7-10, 2021 (virtual meeting).
Petersen KS, et al. A culinary dose of herbs and spices improves 24-hour blood pressure in adults at risk for cardiometabolic diseases: A randomized, crossover, controlled-feeding study. Presented at: American Society of Nutrition Scientific Sessions and Annual Meeting; June 7-10, 2021 (virtual meeting).
Rosas M, et al. Effects of fresh mango consumption on blood glucose, insulin, and other cardiovascular disease risk factors in overweight and obese adults. Presented at: American Society of Nutrition Scientific Sessions and Annual Meeting; June 7-10, 2021 (virtual meeting).
A fermented-food diet increases microbiome diversity and lowers inflammation, Stanford study finds
Stanford researchers discover that a 10-week diet high in fermented foods boosts microbiome diversity and improves immune responses.JUL 122021
Stanford researchers found that eating a diet high in fermented foods such as kimchi increases the diversity of gut microbes, which is associated with improved health. Nungning20/Shutterstock
A diet rich in fermented foods enhances the diversity of gut microbes and decreases molecular signs of inflammation, according to researchers at the Stanford School of Medicine.
In a clinical trial, 36 healthy adults were randomly assigned to a 10-week diet that included either fermented or high-fiber foods. The two diets resulted in different effects on the gut microbiome and the immune system.
Eating foods such as yogurt, kefir, fermented cottage cheese, kimchi and other fermented vegetables, vegetable brine drinks, and kombucha tea led to an increase in overall microbial diversity, with stronger effects from larger servings. “This is a stunning finding,” said Justin Sonnenburg, PhD, an associate professor of microbiology and immunology. “It provides one of the first examples of how a simple change in diet can reproducibly remodel the microbiota across a cohort of healthy adults.”
In addition, four types of immune cells showed less activation in the fermented-food group. The levels of 19 inflammatory proteins measured in blood samples also decreased. One of these proteins, interleukin 6, has been linked to conditions such as rheumatoid arthritis, Type 2 diabetes and chronic stress.
“Microbiota-targeted diets can change immune status, providing a promising avenue for decreasing inflammation in healthy adults,” said Christopher Gardner, PhD, the Rehnborg Farquhar Professor and director of nutrition studies at the Stanford Prevention Research Center. “This finding was consistent across all participants in the study who were assigned to the higher fermented food group.”
Justin Sonnenburg
Microbe diversity stable in fiber-rich diet
By contrast, none of these 19 inflammatory proteins decreased in participants assigned to a high-fiber diet rich in legumes, seeds, whole grains, nuts, vegetables and fruits. On average, the diversity of their gut microbes also remained stable. “We expected high fiber to have a more universally beneficial effect and increase microbiota diversity,” said Erica Sonnenburg, PhD, a senior research scientist in basic life sciences, microbiology and immunology. “The data suggest that increased fiber intake alone over a short time period is insufficient to increase microbiota diversity.”
The study published online July 12 in Cell. Justin and Erica Sonnenburg and Christopher Gardner are co-senior authors. The lead authors are Hannah Wastyk, a PhD student in bioengineering, and former postdoctoral scholar Gabriela Fragiadakis, PhD, who is now an assistant professor of medicine at UC-San Francisco.
A wide body of evidence has demonstrated that diet shapes the gut microbiome, which can affect the immune system and overall health. According to Gardner, low microbiome diversity has been linked to obesity and diabetes.
“We wanted to conduct a proof-of-concept study that could test whether microbiota-targeted food could be an avenue for combatting the overwhelming rise in chronic inflammatory diseases,” Gardner said.
The researchers focused on fiber and fermented foods due to previous reports of their potential health benefits. While high-fiber diets have been associated with lower rates of mortality, the consumption of fermented foods can help with weight maintenance and may decrease the risk of diabetes, cancer and cardiovascular disease.
Erica Sonnenburg
The researchers analyzed blood and stool samples collected during a three-week pre-trial period, the 10 weeks of the diet, and a four-week period after the diet when the participants ate as they chose.
The findings paint a nuanced picture of the influence of diet on gut microbes and immune status. On one hand, those who increased their consumption of fermented foods showed similar effects on their microbiome diversity and inflammatory markers, consistent with prior research showing that short-term changes in diet can rapidly alter the gut microbiome. On the other hand, the limited change in the microbiome within the high-fiber group dovetails with the researchers’ previous reports of a general resilience of the human microbiome over short time periods.
Designing a suite of dietary and microbial strategies
The results also showed that greater fiber intake led to more carbohydrates in stool samples, pointing to incomplete fiber degradation by gut microbes. These findings are consistent with other research suggesting that the microbiome of people living in the industrialized world is depleted of fiber-degrading microbes.
“It is possible that a longer intervention would have allowed for the microbiota to adequately adapt to the increase in fiber consumption,” Erica Sonnenburg said. “Alternatively, the deliberate introduction of fiber-consuming microbes may be required to increase the microbiota’s capacity to break down the carbohydrates.”
In addition to exploring these possibilities, the researchers plan to conduct studies in mice to investigate the molecular mechanisms by which diets alter the microbiome and reduce inflammatory proteins. They also aim to test whether high-fiber and fermented foods synergize to influence the microbiome and immune system of humans. Another goal is to examine whether the consumption of fermented food decreases inflammation or improves other health markers in patients with immunological and metabolic diseases, and in pregnant women and older individuals.
Christopher Gardner
“There are many more ways to target the microbiome with food and supplements, and we hope to continue to investigate how different diets, probiotics and prebiotics impact the microbiome and health in different groups,” Justin Sonnenburg said.
Other Stanford co-authors are Dalia Perelman, health educator; former graduate students Dylan Dahan, PhD, and Carlos Gonzalez, PhD; graduate student Bryan Merrill; former research assistant Madeline Topf; postdoctoral scholars William Van Treuren, PhD, and Shuo Han, PhD; Jennifer Robinson, PhD, administrative director of the Community Health and Prevention Research Master’s Program and program manager of the Nutrition Studies Group; and Joshua Elias, PhD.
Researchers from Chan-Zuckerberg Biohub also contributed to the study.
The work was supported by donations to the Center for Human Microbiome Research; Paul and Kathy Klingenstein; the Hand Foundation; Heather Buhr and Jon Feiber; Meredith and John Pasquesi; the National Institutes of Health (grant T32 AI 7328-29); a Stanford Dean’s Postdoctoral Fellowship; a National Science Foundation Graduate Student Fellowship; and seed funding from the Institute for Immunity, Transplantation and Infection and from the Sean N. Parker Center for Allergy and Asthma Research.
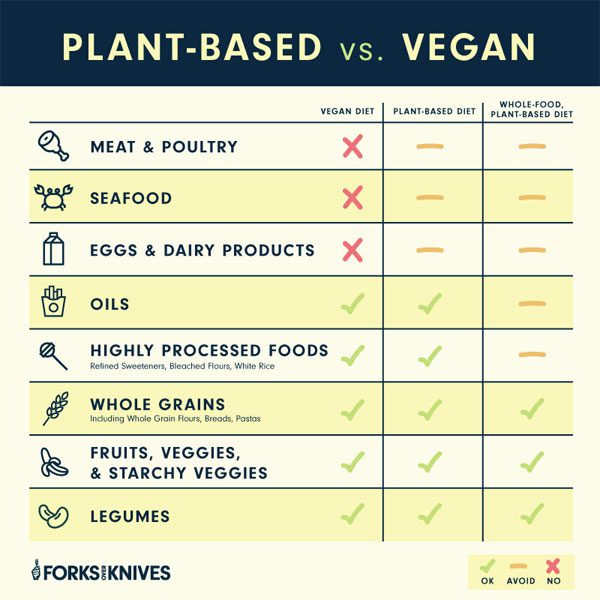
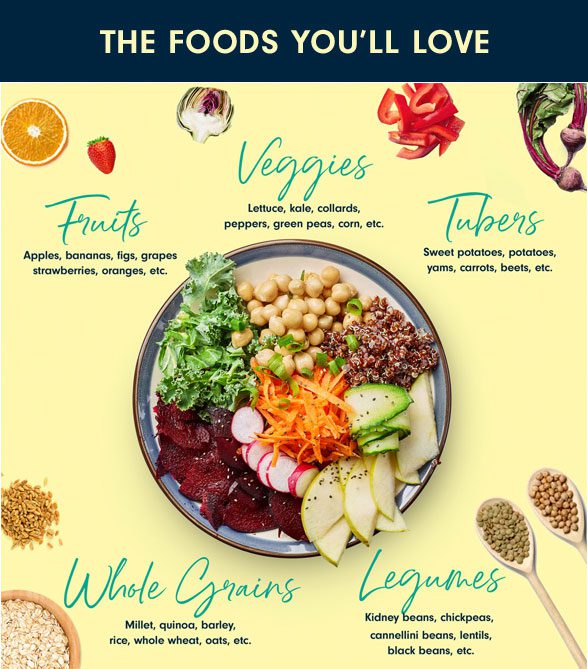
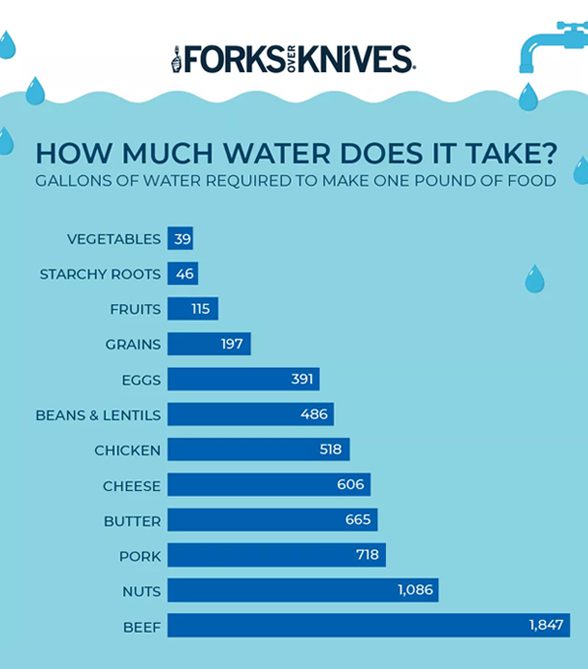




















 Melina B. Jampolis
Melina B. Jampolis




{kind=link}