The GI-MAP (Gastrointestinal Microbial Assay Plus) test, offered by Diagnostic Solutions Laboratory, is a comprehensive stool test designed to assess the microbiome and detect gastrointestinal pathogens.
Utilizing advanced DNA sequencing technology, the GI-MAP provides detailed insights into the presence and levels of gut bacteria, viruses, parasites, and fungi, allowing for targeted interventions to restore gut health.
This test also offers a comprehensive assessment of gastrointestinal function, to aid in assessment and management of various digestive disorders including irritable bowel syndrome (IBS), inflammatory bowel disease (IBD), and gastrointestinal infections. [20.]
The GI-MAP test analyzes over 40 different commensal and pathogenic microorganisms, including bacteria, viruses, parasites, and fungi, along with markers of inflammation and digestive function. By identifying specific pathogens and imbalances in the gut microbiome, the GI-MAP offers valuable information for healthcare providers to develop personalized treatment plans tailored to the individual’s unique microbial profile.
This stool test offers a non-invasive and comprehensive approach to evaluating gut health, providing actionable insights to optimize digestion, immune function, and overall well-being. With its ability to detect a wide range of gastrointestinal pathogens and dysbiosis, the GI-MAP test serves as a valuable tool in the assessment and management of digestive disorders, allowing for targeted interventions to promote gut health and improve patient outcomes.
If you want to order the Zonulin add-on, please order the “GI-MAP + Zonulin” test. The GI-MAP measures a variety of gastrointestinal microbiota DNA using qPCR technology. It detects microbial imbalance, microbes contributing to illness, and indicators of digestion, absorption, inflammation, and immune function. Due to a supply shortage, this test no longer includes antibiotic resistance genes to opportunistic/universal bacteria.
Ordering the GI-MAP® – GI Microbial Assay Plus
The GI-MAP® from Diagnostic Solutions Laboratory is a comprehensive stool analysis that measures gastrointestinal microbiota DNA from a single stool sample. Using state-of-the-art, quantitative polymerase chain reaction (qPCR) technology, the GI-MAP evaluates gut pathogens, bacterial infections, yeast overgrowth, viruses, and parasites. Antibiotic resistance genes and virulence factors are also included on the test for unparalleled insight into H. pylori.
Recently, the GI-MAP has been enhanced to include an upgraded report with visual cues that allow for easier readability. Further, additional markers, including Roseburia spp., Desulfovibrio spp., and Eosinophil Activation Protein (EPX/EDN), have been added to include even greater insight into patient health.
The GI-MAP was designed to detect microbes that may be disturbing normal microbial balance or contributing to illness. To complete the picture of overall health, the GI-MAP includes key markers related to digestion, absorption, inflammation, and immune function.
An unhealthy gut can cause uncomfortable symptoms that are felt beyond the gastrointestinal (GI) tract. In fact, the root cause of brain fog, fatigue, headaches, food sensitivities, and more can often be traced back to the gut.
The GI-MAP offers impactful, quantitative results that enable practitioners to create personalized protocols that address the underlying cause(s) of uncomfortable symptoms for even the most complex patients.
Why Is Quantification Using qPCR Technology So Important?
qPCR offers a much more accurate way to detect and quantify clinically-relevant organisms than standard PCR, culture, microscopy, or DNA sequencing-based methods. Accurately assessing how much
of an organism’s DNA is present in a patient’s stool sample is essential for helping practitioners to determine the clinical significance of pathogenic organisms and dysbiosis patterns.
GI-MAP Allows for the Personalized Gut-Healing Treatment Plans
The GI-MAP allows practitioners to create personalized treatment protocols to address gut dysfunction based on which infections are urgent, which areas of the gut are already optimized, and which areas should be addressed after an infection is resolved.
Additionally, the quantification offers a remarkable ability to see how treatment modalities are working because a retest after treatment can show whether a parasite has resolved, dysbiosis has improved, and more.
What is Included in the GI-MAP?
The GI-MAP Test by Diagnostic Solutions Laboratory is a comprehensive stool test that uses quantitative PCR technology to detect bacteria, parasites, fungi, viruses, and more within the gastrointestinal tract. The test is designed to provide insight into the microbiome’s composition, the presence of pathogenic microorganisms, and other important markers of gastrointestinal health. Here’s a summary of what the GI-MAP can show:
Microbial Flora Analysis
Pathogens: bacterial, parasitic and viral pathogens are known causes of intestinal gastroenteritis. The presence and amount of these pathogens are reported when found. It is important to note that some patients may test positive for these pathogens, yet be asymptomatic. It is possible for these pathogens to be present in the digestive tract but not actively produce virulence factors, which cause symptoms.
Specific pathogens Reported on the GI-MAP are:
Bacterial Pathogens:
Campylobacter
C. difficile Toxin A
C. difficile Toxin B
Enterohemorrhagic E. coli
E. coli O157
Enteroinvasive E. coli/Shigella
Enterotoxigenic E. coli LT/ST
Shiga-like Toxin E. coli stx1
Shiga-like Toxin E. coli stx2
Salmonella
Vibrio cholerae
Yersinia enterocolitica
Parasitic Pathogens:
Cryptosporidium
Entamoeba histolytica
Giardia
Viral Pathogens:
Adenovirus 40/41
Norovirus GI/II
H. Pylori: as with other gastrointestinal pathogens, it is possible to harborthe bacteria H. pylori and be asymptomatic. H. pylori typically invades the stomach or the duodenum. It is linked to ulcers, chronic gastritis, and stomach cancer, as well as causing initial low stomach acid followed by hyperaciduria, often leading to heartburn or GERD (gastrointestinal reflux disease). It may also be a culprit behind dyspepsia, abdominal pain, nausea, vomiting and chronic gastrointestinal symptoms.
By using DNA analysis for H. pylori virulence factors, the GI-MAP can represent the genetic potential for a particular H. pylori strain to cause pathology. This information, along with the patient’s personal and/or family history, may guide treatment decisions. [2.,4., 9., 10., 17., 18., 24.
Beneficial Bacteria: these are labeled “Commensal/Keystone Bacteria” on the GI-MAP because of their positive benefits on human health. High levels of beneficial bacteria are generally good, indicating a healthy gut microbiome.
These bacteria promote nutrient absorption from food, produce some vitamins (biotin and vitamin K), maintain a healthy mucosal lining, support detoxification, regulate immune function and inflammation at the gut lining, and protect against colonization from potential pathogens. [7.] Low levels might suggest a need for dietary changes, probiotics, or prebiotics.
Specific Commensal/Keystone Bacteria Reported on the GI-MAP Are:
Bacteroides fragilis
Bifidobacterium spp.
Enterococcus spp.
Escherichia spp.
Lactobacillus spp.
Enterobacter spp.
Akkermansia muciniphila
Faecalibacterium prausnitzii
Roseburia spp.
The GI-MAP also reports the following bacterial phyla, or groups of bacteria, and their ratio:
Bacteroidetes
Firmicutes
Firmicutes:Bacteroidetes Ratio
Bacteroidetes, a gram-negative group of bacteria, and Firmicutes, a gram-positive group of bacteria, constitute the two major groups of bacteria that are present in the human microbiome. An abnormal result in one or both of these phyla indicates an imbalance in the individual’s microbiome.
An increased Firmicutes:Bacteroidetes ratio indicates a microbial imbalance that has been implicated in increased caloric extraction from food causing weight gain and obesity; decreased insulin sensitivity; and increased inflammation. [14.]
A high Firmicutes:Bacteroidetes ratio may signal the need to make dietary improvements, provide digestive support, and individualized probiotic recommendations when taken into consideration with the rest of the findings of the GI-MAP.
Opportunistic Bacteria: These are not harmful in small amounts but can cause issues if overgrown, especially in immune-compromised patients and/or in patients with leaky gut or impaired intestinal lining integrity. They have been known to cause symptoms in some people including diarrhea, loose stool, abdominal pain, and constipation, and some strains have been linked with autoimmune conditions. [5., 20.] High levels may indicate dysbiosis or an imbalance in the gut microbiota.
Specific Opportunistic Bacteria Reported on the GI-MAP Are:
Fungi/Yeast: fungal organisms are a common component of the human microbiome, but overgrowth can cause problems, especially in the setting of leaky gut or an impaired intestinal lining. In patients who have positive findings for these organisms, additional testing including urinary D-arabinitol or Candida antibodies may be warranted.
Fungi/Yeast Reported on the GI-MAP Are:
Candida spp.
Candida albicans
Geotrichum spp.
Microsporidium spp.
Rhodotorula spp.
Viruses: the presence of CMV (cytomegalovirus) and EBV (Epstein-Barr virus) in stool has been correlated with IBD. [8., 18.]. IBD patients infected with these viruses may be more susceptible to IBD flare ups with viral reactivations. [16.] A positive finding on the GI-MAP indicates current infection.
Viruses Reported on the GI-MAP Are:
CMV, Cytomegalovirus
EBS, Epstein-Barr Virus
Parasites: parasites are organisms that feed on the host organism, at its expense. The GI-MAP tests for pathogenic and non-pathogenic parasites.
Parasites Reported on the GI-MAP Are:
Protozoa
Blastocystis hominis
Chilomastix mesnili
Cyclospora spp.
Dientamoeba fragilis
Endolimax nana
Entamoeba coli
Pentatrichomonas hominis
Worms
Ancylostoma duodenale
Ascaris lumbricoides
Necator americanus
Trichuris trichiura
Taenia spp.
Digestive Markers
Elastase: Elastase 1 is a digestive enzyme produced exclusively by the pancreas, making it an effective indirect marker of pancreatic function. Elastase levels are not affected by the use of supplemental digestive enzymes. Elastase helps break down proteins. Low levels can indicate pancreatic insufficiency.
Steatocrit: Steatocrit is fecal fat. Normally, dietary fat in the small intestine is emulsified by bile acids and absorbed. High levels suggest fat maldigestion and/or malabsorption, which can be due to various digestive disorders.
Inflammatory and Immune Markers
Calprotectin: considered the “gold standard” marker of inflammation in the GI tract. High levels can indicate inflammatory bowel diseases (IBD) such as Crohn’s disease or ulcerative colitis, and is used to distinguish IBD from irritable bowel syndrome, IBS, in which no pathological process can be determined; instead, IBS is considered a functional diagnosis.
Secretory IgA (sIgA): the primary immunoglobulin at the digestive system border, sIgA is an immune marker that plays a critical role in mucosal immunity. Levels can provide insight into the immune system’s status in the gut, with elevated levels indicating an acute infection and/or chronic dysbiosis, food sensitivities, or acute stress. Low levels may be caused by chronic stress, immune compromise, and again, chronic dysbiosis.
Anti-Gliadin SIgA: gliadin is a component of gluten, which can stimulate inflammation in the digestive tract of susceptible individuals. It may indicate an immune response to gluten in the digestive tract, although this does not necessarily correlate with blood levels.
Eosinophil Activation Protein (EDN/EPX): eosinophils are white blood cells normally present in the gut that support immunity and maintain the protective mucosal barrier of the gut lining. [15.] The Eosinophil Activation Protein is secreted by eosinophils in response to infections (particilularly viral infections), allergic and inflammatory responses. [1.]
Additional Markers
Occult Blood: The presence of blood in the stool that is not visible to the eye can indicate bleeding in the GI tract.
Beta-Glucuronidase: high levels of beta-glucuronidase in the stool indicates dysbiosis, and it may also point to detoxification issues at the liver, specifically with the glucuronidation step of phase II liver detoxification. Rising levels of Beta-GLucuronidase have also been correlated with impaired estrogen metabolism and increased risk of estrogen-induced diseases. [13.]
Antibiotic Resistance Genes: Detection of these genes can help guide treatment decisions, specifically whether antibiotic therapy is warranted in a particular case, and which antibiotics may not be effective against certain bacteria.
Zonulin Add-On Test
Zonulin is available as an add-on marker on the GI-MAP. Adding a Zonulin test enhances the comprehensiveness of the GI-MAP by providing additional information about gut health beyond microbial composition.
Zonulin is a protein involved in modulating the tight junctions between epithelial cells in the intestines. Elevated levels of zonulin can indicate increased intestinal permeability, often referred to as “leaky gut syndrome.” Incorporating a Zonulin test alongside the GI-MAP allows clinicians to assess the integrity of the intestinal barrier, providing insights into gastrointestinal health and potential underlying conditions such as inflammatory bowel disease, celiac disease, and autoimmune disorders.
Who Can Benefit from a GI-MAP Comprehensive Stool Analysis Test?
The GI-MAP test, with its comprehensive analysis of gut health, is beneficial for a wide range of individuals from those looking to optimize their overall health to individuals who have been struggling with chronic illnesses with or without a clear diagnosis. Here’s a breakdown of who can benefit from a GI-MAP test:
Individuals Seeking to Optimize Health: even in the absence of symptoms, the GI-MAP can offer insights into the gut microbiome’s health, providing an opportunity for preventative measures against potential health issues and supporting the body’s natural processes.
Patients with Chronic Digestive Dysfunction: for those who have suffered from chronic symptoms with or without a clear diagnosis, the GI-MAP can help identify underlying imbalances or infections in the gut that may be contributing to their health issues.
Autoimmune Diseases: since gut health is closely linked to the immune system, identifying and addressing gut dysbiosis can provide additional treatment options and provide crucial support in managing autoimmune conditions. [5., 20., 22.]
Gastrointestinal Disorders: for patients struggling with Small Intestinal Bowel Overgrowth (SIBO), Irritable Bowel Syndrome (IBS) and Inflammatory Bowel Disease (IBD), the GI-MAP can identify specific pathogens, inflammatory markers, and digestive imbalances that may be contributing to symptoms like gas, bloating, diarrhea, and constipation. [20., 25.]
Digestive Complaints: people experiencing unexplained digestive issues such as gas, bloating, heartburn, indigestion, diarrhea, or constipation can identify potential causes and receive targeted treatment recommendations.
Neurological and Cognitive Issues: the vagus nerve is the primary nerve that innervates the digestive tract, and is considered the “highway of the gut-brain axis”. Insights into the gut-brain axis through the GI-MAP may reveal how gut health impacts an individual’s cognitive function and affects memory, concentration, and brain fog. [12.]
Skin Conditions: conditions like acne and psoriasis have been linked to gut health. Identifying and addressing gut dysbiosis can be a part of a comprehensive treatment plan to improve and restore skin health. [11.]
Mood Disorders: the gut-brain connection means that imbalances in gut microbiota can impact mood and emotional well-being, making the GI-MAP valuable for individuals with these conditions. [12., 21.]
Metabolic and Weight Issues: The GI-MAP can offer insights into the role of the gut microbiome in metabolism and weight regulation, providing avenues for intervention in diabetes management and weight loss. [3., 6.]
The GI-MAP test is a versatile tool that can benefit a broad spectrum of individuals by providing a detailed look at gut health and its impact on overall well-being. By identifying specific imbalances and pathogens, it allows for targeted interventions that can significantly improve a person’s quality of life, especially for those dealing with chronic and elusive health issues.
Functional medicine is a personalized, systems-oriented approach to healthcare that aims to identify and address the root causes of disease, rather than just treating symptoms. It views the body as an interconnected system, not a collection of independent organs divided by specialties. This model integrates both conventional and alternative medical practices, and emphasizes lifestyle, nutrition, and environmental factors.
🔬 Core Principles of Functional Medicine
Principle
Description
Patient-centered care
Focuses on the individual, not just the disease. Emphasizes therapeutic partnerships between patient and practitioner.
Biochemical individuality
Recognizes that genetic and environmental factors create unique expressions of health and disease for each individual.
Systems biology approach
Addresses how systems in the body (hormonal, digestive, immune, detoxification, etc.) are interrelated and influence each other.
Dynamic balance
Seeks to restore balance among internal and external factors, including nutrition, sleep, stress, movement, and relationships.
Root cause resolution
Aims to identify the underlying dysfunctions that contribute to chronic illness (e.g., inflammation, oxidative stress, gut dysbiosis).
Integrative and science-based
Draws on both traditional Western medicine and alternative treatments backed by evidence.
🔄 The Functional Medicine Matrix
A core tool used in practice is the IFM Functional Medicine Matrix, developed by The Institute for Functional Medicine (IFM). It helps clinicians organize a patient’s history and identify clinical imbalances in:
Assimilation (e.g., digestion, microbiome)
Defense and repair (e.g., immune function, inflammation)
Energy (e.g., mitochondrial function)
Biotransformation and elimination (e.g., detox pathways)
Communication (e.g., hormones, neurotransmitters)
Transport (e.g., cardiovascular and lymphatic systems)
Summary: Offers a matrix and timeline-based approach for systemic root cause evaluation. Strong emphasis on patient engagement, personalized plans, and lifestyle medicine.
Textbook of Functional Medicine – IFM, 2005.
Summary: Comprehensive reference covering the conceptual and clinical applications of functional medicine, including diagnostic approaches and treatment frameworks.
David S. Jones et al., “Functional Medicine: The Future of Chronic Disease Management” (Nutrition in Clinical Practice, 2010)
Summary: Reviews the rationale and implementation of functional medicine for chronic disease care, highlighting its systems-based, patient-focused, and evidence-informed methodology.
James Maskell. The Evolution of Medicine (2016) – Overview of how functional and integrative medicine are changing primary care.
Summary: Emphasizes prevention and personalized care, discusses challenges to conventional care models, and explores scalable functional medicine solutions.
🧠 In Summary
Functional medicine is a science-based, integrative discipline that seeks to optimize health by identifying and treating underlying dysfunctions through individualized and holistic care plans. It is especially valuable in chronic disease management, where conventional medicine often fails to address multifactorial causes.
You said:
Functional Medicine Labs to Test for Root Causes of Hyperglycemia
Patients with hyperglycemia are often diagnosed incidentally through a routine wellness panel consisting of a complete blood count (CBC), comprehensive metabolic panel (CMP), and thyroid panel. These panels evaluate blood cells, blood sugar, electrolyte balance, and liver, kidney, and thyroid function. They are helpful labs for patients with hyperglycemia and diabetes to rule out underlying infections and hyperthyroidism, monitor kidney health, and assess blood pH.
Additional functional labs can help to better get to the root cause of hyperglycemia and diabetes, making treatment protocols more effective. Functional doctors commonly order the following labs for patients with hyperglycemia and diabetes.
Diabetes Panel
A diabetes panel offers a more accurate assessment of hyperglycemia and diabetes by measuring multiple markers associated with glucose metabolism, including the most common biomarkers: glucose, hemoglobin A1c, and insulin.
While these biomarkers are valuable, this panel lacks the ability to track blood glucose levels in real-time. This is why many functional practitioners turn to continuous glucose monitoring (CGM) These sensors that monitor glucose levels in the interstitial fluid every five minutes. The glucose patterns obtained through CGM better inform individuals and their doctors about how diet, physical activity, and medications/supplements influence glycemic control.
Adrenal Function
Cortisol can be measured through serum, saliva, or urine. While serum and urinary cortisol are preferred to rule out pathologic disorders related to adrenal function (e.g., Cushing’s), salivarycortisol is preferred by functional doctors to evaluate functional disorders related to the stress axis.
Genetic Panel
Genetic factors may mediate alterations in glucose homeostasis. A genetic panel assesses for genetic variations that influence the efficacy of insulin and glucose pathways in the body and can predispose an individual to type 1 and 2 diabetes mellitus.
Functional Medicine Labs That Can Help Individualize Treatment Options for Patients With Hyperglycemia
Functional labs can help doctors personalize dietary, lifestyle, and supplemental treatment options. The following labs could be considered on an individual basis for patients struggling with hyperglycemia.
Micronutrient Panel
Nutritional deficiencies associated with high blood sugar and insulin resistance include inositol, vitamin D, magnesium, zinc, and chromium (2). A micronutrient panel can identify deficiencies or insufficiencies of these (and other) essential nutrients that may contribute to poor glucose control and health outcomes.
Comprehensive Stools testing
Numerous studies have examined the human gut microbiota in relation to type 2 diabetes. The data from these studies suggest gut bacteria directly affect the mechanisms underlying the development of type 2 diabetes and that intestinal dysbiosis contributes to blood sugar dysregulation and hyperglycemia. Additionally, intestinal hyperpermeability and digestive dysfunction can contribute to immune dysregulation, systemic inflammation, and nutrient deficiencies associated with type 1 diabetes, glucose metabolism, and poor cardiovascular outcomes. Therefore, a comprehensive stool analysis can be valuable to thoroughly evaluate gastrointestinal health as it pertains to whole-body functioning.
Sleep Assessment
The sleep-stress cycle refers to the bidirectional relationship between the two and how they affect each other. High stress and cortisol negatively impact sleep by dysregulating the body’s circadian rhythm. Poor sleep, in turn, sustains cortisol hypersecretion and the psychoemotional perception of stress. This sleep-stress cycle can quickly perpetuate hyperglycemia.
In addition to a functional salivary cortisol test (discussed above), ordering a sleep study and measuring melatonin, the body’s master sleep hormone, can help to unravel the sleep-stress cycle.
Integrating Testing, Lifestyle Modifications, and Integrative Therapies
The importance of personalized approaches in managing high blood sugar cannot be overstated. Every individual’s response to treatment, underlying health conditions, and lifestyle factors can vary significantly. By adopting personalized approaches that consider test results and the patient’s goals, preferences, and unique circumstances, healthcare providers can tailor interventions to optimize outcomes. By combining the expertise of different healthcare disciplines, patients can benefit from a comprehensive treatment plan that integrates conventional medical interventions with lifestyle modifications, dietary changes, stress management techniques, and other complementary therapies. Such an approach empowers patients to actively participate in their care and increases the likelihood of achieving desired health outcomes in managing high blood sugar.
Conventional Treatment for Hyperglycemia
The treatment goals of hyperglycemia involve controlling blood sugar, eliminating symptoms related to high blood sugar, and preventing long-term complications. Depending on the cause of hyperglycemia, different conventional approaches may need to be taken. These approaches often incorporate diet and lifestyle counseling, oral glucose-lowering medications, and insulin therapy. (1)
Nutrition for Hyperglycemia
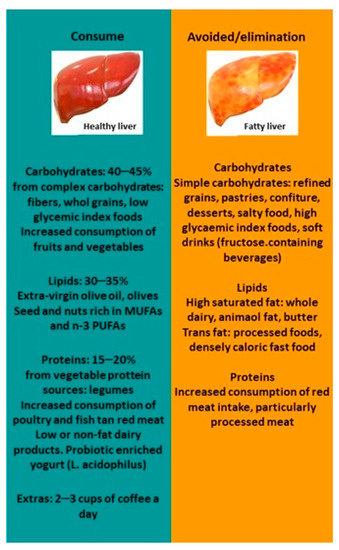
Nutrition plays a critical role in managing hyperglycemia. Dietary choices can prevent high blood sugar spikes and help the body return to a healthy baseline after eating. Processed foods rich in simple carbohydrates, added sugars, and unhealthy fats contribute to the development of insulin resistance and rapid spikes in blood sugar. Alternatively, well-balanced meals composed of healthy ratios of complex carbohydrates, fiber, lean proteins, and unsaturated fats lead to steadier blood sugars, improved insulin sensitivity, and increased satiety (helping to curb sugar cravings and overeating). Evidence-based, anti-inflammatory, and low-glycemic dietary patterns proven to support healthy blood sugar levels include the Mediterranean, DASH, low-carbohydrate, and plant-based diets. (8)
Supplements and Herbs for Hyperglycemia
Several supplements have been shown to decrease blood sugar levels and can be added to a treatment plan in addition to lifestyle and dietary modifications to expedite treatment success.
Berberine
Berberine is a naturally occurring plant compound with antimicrobial, anti-inflammatory, anti-lipidemic, and hypoglycemic properties. A meta-analysis of 27 randomized controlled trials and over 2,500 patients found that supplemental berberine increased the therapeutic effects of lifestyle modifications, dietary changes, and oral diabetes medications. Positive clinical outcomes noted in this meta-analysis included reductions in fasting glucose, post-prandial glucose, and hemoglobin A1c.
Cinnamon
Cinnamon is a common household pantry spice that has medicinal properties. The active component of cinnamon, cinnamaldehyde, has been attributed to positive glucose-managing effects. It is believed that cinnamaldehyde promotes insulin release and enhances insulin sensitivity, promoting cellular uptake by cells. Studies have shown that therapeutic doses of cinnamon decrease fasting blood sugar levels. (9)
Chromium
Chromium has been shown to enhance insulin’s metabolic effect; chromium deficiency has been linked to type 2 diabetes. A meta-analysis of 28 studies revealed that oral chromium supplementation significantly reduces fasting blood sugar, insulin levels, hemoglobin A1c, and HOMA-IR (a marker of insulin resistance).
Gymnema
Gymnema is an interesting herb thought to act by multiple mechanisms to lower blood sugar levels successfully. Perhaps the most interesting characteristic of this herb is its ability to interfere with perceiving the sweet taste; by inhibiting the sweet taste of foods, people may naturally limit their intake of sweet foods. Additionally, gymnema decreases gastrointestinal absorption of sugar, stimulates pancreatic insulin production, and improves signaling for peripheral uptake of blood glucose. Research has shown that the culmination of these properties reduces fasting blood sugar and hemoglobin A1c levels. (10)
Exercise for Managing High Blood Sugar
Exercise offers numerous benefits for managing high blood sugar and is crucial to diabetes management. Regular physical activity helps improve insulin sensitivity, allowing the body to utilize glucose for energy effectively. It also promotes weight loss or weight management, reducing the risk of insulin resistance. Engaging in exercise can lower blood sugar levels, enhance cardiovascular health, and decrease the risk of developing complications associated with diabetes. (11)
The American Heart Association (AHA) recommends incorporating aerobic and anaerobic forms of exercise into your physical routine to promote cardiovascular health and prevent insulin resistance. It is recommended to gradually work up to at least 150 minutes of moderate-intensity or 75 minutes of high-intensity aerobic activity, with at least two sessions of muscle-strengthening exercise, every week.
Beginning a new exercise routine can feel overwhelming. The good news is that research shows even small amounts of physical activity are better than none. For example, walking 15 minutes after meals significantly helps 24-hour glucose control.
Stress Management and Quality Sleep for Hyperglycemia
As discussed earlier, chronic stress and lack of sleep contribute to sustained elevations in cortisol and poorer blood sugar control. Research has shown that diabetic patients who feel stressed also report greater insulin use, poorer glycemic control, and a general sense of less empowerment. Therefore, ensuring patients can implement effective stress management techniques and get adequate good-quality sleep is a very important aspect of a hyperglycemia treatment protocol.
In addition to eating a healthy, well-balanced diet and exercising regularly, mindfulness-based stress reduction practices (discussed in more detail below) and adaptogenic herbs can modulate the “fight-or-flight” division of the nervous system and cortisol levels to help the body better adapt to stress.
Establishing healthy sleep hygiene habits can promote restorative sleep. The following tips are often recommended to facilitate deep sleep. Aim to wake up and go to bed at the same time each day of the week. Avoid intense activity and other stimulants (e.g., caffeine) later in the afternoon and evening. Create a calming wind-down routine before bed that includes dimming lights and avoiding blue light. Ensure your bedroom is dark, cool, and quiet.
Mind-Body Approaches for Hyperglycemia Management
Mind-body therapies, including yoga, mindfulness-based stress reduction therapy, and acupuncture, effectively manage stress. Interestingly, research demonstrates that each of these modalitiessupports healthier blood sugar control, indicated by improvements in fasting blood glucose and hemoglobin A1c levels.
Order from 30+ labs in 20 seconds (DUTCH, Mosaic, Genova & More!)
We make ordering quick and painless — and best of all, it’s free for practitioners.
Summary
Hyperglycemia is a medical condition that cannot go unrecognized and untreated. An integrative approach to prevent and treat high blood sugar, incorporating functional medicine labs and a combination of complementary therapeutic modalities, offers promising possibilities for achieving optimal glycemic control.
The information provided is not intended to be a substitute for professional medical advice. Always consult with your doctor or other qualified healthcare provider before taking any dietary supplement or making any changes to your diet or exercise routine.
Ever since the dawn of the 21st century, the concept of total healthcare has transformed to include, besides physical fitness, wholesome diets, mental wellness and sleep hygiene, one more rather vital component.
That is, attaining the very desirable fountain of youth – a visibly vibrant appearance sans any signs of ageing.
And this is something that, for most people, is certainly easier said than done. Chiefly owing to the heightened stress from hectic schedules, be it at home or work, constant exposure to pollutants, germs in external environments, households, along with harsh UV rays in sunlight, directly damaging the skin.
These harmful factors invariably result in wrinkles, dark patches, loss of volume, elasticity, fine lines, scarring, prominent tans, grooves and sagging, leading to a dull, lifeless, sunken look to the face.
Although these problems might be inherently modern, the solutions for acquiring smooth, soft, and radiant skin can be found in the age-old Ayurvedic scriptures.
How To Slow Down Skin Ageing, As Per Ayurveda:
Ayurveda – the ancient Indian system of medicine, comprises tomes of information on skin-reviving herbs in the archaic texts, namely Charaka Samhita, Atharva Veda and Sushruta Samhita. These classical manuscripts define the primary requirements for skin health as:
Regulating Kapha Dosha: By providing adequate moisture, eliminating dryness in skin.
Controlling Pitta Dosha: By guaranteeing optimal metabolism, hormone function of skin tissues.
Maintaining Vata Dosha: By conserving proper blood circulation, nutrient supply to the skin.
Wellness Of Three Dhatus:
The three dhatus or body tissues crucial for fortifying skin consist of:
Rasa: This refers to the nutritional fluids that foster luminous skin.
Rakta: This is the key element of nourished blood that purifies the skin of toxins.
Mamsa: These are the strong muscles that offer structural support to the skin.
Types Of Therapies:
Ayurveda vouches for holistic rejuvenation of skin tissues through two forms of anti-ageing medications:
Urjaskara: Coming from the Sanskrit words “Urjas” meaning strength and “Kara” meaning to give, this deals with the promotive and preventive aspects, to enrich texture for gorgeous skin.
Vyadhihara: Derived from Sanskrit, where “Vyadhi” translates to illness and “Hara” implies to defeat, this encompasses efficacious methods to completely treat a host of skin ailments.
Classes Of Herbs:
According to the traditional Ayurvedic documents, there exist eight categories of skin-related rasayana or invigorating anti-ageing herbs:
Vayasthapana: This group of herbs helps to defy growing older, literally meaning upholding youthfulness or ceasing ageing.
Varnya: These herbs significantly brighten the complexion of the skin.
Sandhaniya: This category of herbs repairs wear and tear, stimulates regenerative functions of the skin.
Vranaropana: These potent herbs heal the deeper layers of skin.
Tvachya: These herbs deliver hydration and moisture to the skin.
Shothahara: Packed with anti-inflammatory traits, these herbs protect skin from detrimental chemicals, allergens.
Tvachagnivardhani: These herbs infuse shine and lustre to the skin, by promoting its intrinsic metabolism.
Tvagrasanaya: These herbs refine skin features by averting chronic ailments.
Rejuvenating Natural Remedies For Youthful, Glowing Skin:
Gotu Kola (Asiatic Pennywort)
Abundant in the powerful antioxidant triterpenes – asiaticoside and madecassic acid, gotu kola, also called mandukaparni, is a wonderful therapy for diminishing acne, scars and injuries on the skin.
Dry a bunch of gotu kola leaves, powder it and mix it with some honey. Apply a small portion on regions of skin with pimples, to reduce swelling and redness.
Amla or amalaki is renowned for the treasure trove of beneficial constituents it houses, for the wellbeing of the skin, such as vitamin C, gallic acid and tannins. Being adaptogenic, they safeguard skin from excess stressors, pressure.
Dab some diluted amla juice on the face, leave it on for 10 minutes and wash off with lukewarm water, for rested skin sans wrinkling, drooping.
Chandan (Sandalwood)
Instilled with a pleasing scent, profuse cooling properties and organic brightening essentials, chandan or shweta chandana remarkably rectifies sun tans, dark spots, efficiently treating uneven skin tone.
Make a paste out of chandan powder and milk, apply a uniform layer on the face after cleansing, let it stay for 15 minutes and rinse off, to obtain a flawless, fair complexion.
Salai (Indian Frankincense)
Salai, otherwise termed as sallaki, is bestowed with anti-inflammatory characteristics. It is one of the best herbal antidotes for mending myriad skin disorders including eczema, psoriasis and rosacea ( not recommended without physician approval)
Smear a bit of gum resin extract of the salai plant on peeling and wounded portions of the skin, keep it on for 5 minutes and wash off with cold water. This assists in curing breakouts and blemishes.( not recommended without physician approval) Also Read: Top 5 Incredible Therapeutic Uses Of Indian Frankincense
Gulab (Rose Plant)
Famed for its enticing fragrance, gulab, also known as shatapatri, holds vast reserves of hydrating phytonutrients, besides vitamins A and B complex. These contribute towards locking in moisture, boosting collagen synthesis and nurturing skin integrity.
Gently spread a watery preparation with the essence of rose petals on rough, faded areas of skin, to instantly tone and moisturize the face.( not recommended without physician approval) Here are two herbal face packs for oily skin and dry skin, to banish all skin woes and attain gorgeous youthful looks with pure natural infusions.( not recommended without physician approval)
Ashwagandha (Indian Ginseng):
Ashwagandha reigns as an adaptogenic herb celebrated for its ability to combat stress, a significant contributor to premature ageing. Rich in antioxidants, it neutralises free radicals, promoting cellular vitality and supporting a youthful complexion.( not recommended without physician approval)
Turmeric (Curcuma longa):
Turmeric, with its active compound curcumin, boasts potent anti-inflammatory and antioxidant prowess. A revered spice in Ayurveda, it aids in maintaining skin elasticity, reducing fine lines, and promoting a radiant complexion.( not recommended without physician approval)
Shatavari (Asparagus racemosus):
Shatavari, revered as a feminine tonic, supports overall well-being, including skin health. Its antioxidant-rich composition assists in maintaining a youthful glow, and its adaptogenic properties contribute to hormonal balance.( not recommended without physician approval)
Besan And Chandan Face Pack For Dry Skin:
Ingredients:
2 tbsp besan
2 tsp sandalwood powder
1 tbsp curd
Method:
Combine the besan, chandan and curd in a clean bowl to obtain a homogenous thick paste.
Smear on a uniform layer on the face and neck and keep it on for 15 minutes.
Rinse off with cold water and gently pat dry with a soft towel.( not recommended without physician approval)
How It Works:
Besan is a superb cleansing agent that removes all dust, dirt, grime from the skin, while chandan possesses brightening properties that help diminish age spots, acne scars, uneven skin tone for a younger-looking complexion. Curd is a brilliant moisturiser that infuses hydration into drying, peeling tissues and repairs damaged areas, to bestow smooth, nourished skin.
Multani Mitti And Gulab Face Pack For Oily Skin
Ingredients:
3 tbsp multani mitti i.e. fuller’s earth
1 tbsp tomato juice
4 tsp gulab jal i.e. rose water
Method:
Mix the multani mitti, tomato juice and rose water in a dish such that a fine flowing paste forms.
Apply this blend all over the face and neck, let it stay for 20 minutes until it entirely dries up and the components are absorbed into the skin.
Wash it off completely with lukewarm water. Use this herbal remedy twice a week for best results.
( not recommended without physician approval)
How It Works:
Multani mitti is imbued with numerous minerals being a clay extract and is hence an excellent detoxifying as well as an exfoliating compound that eliminates all impurities, and dead cells from the skin. Tomato juice is rich in vitamin C and the antioxidant lycopene which rejuvenate skin surface, while also holding valuable astringent qualities to shrink large pores on the face and nose for a soft texture and youthful glow. Rose water is a fantastic natural toner that balances the skin’s pH, sebum/oil levels and minimises the appearance of wrinkles, and fine lines.
References:
Critical review of Ayurvedic Varṇya herbs and their tyrosinase inhibition effect – By Khemchand Sharma, Namrata Joshi, and Chinky Goyal
The content provided here is for informational purposes only. This blog is not intended to substitute for medical advice, diagnosis, or treatment. Always seek the advice of a qualified healthcare provider for any questions or concerns you may have regarding a medical condition. Reliance does not endorse or recommend any specific tests, physicians, procedures, opinions, or other information mentioned on the blog.
Disclaimer:
The content provided here is for informational purposes only. This blog is not intended to substitute for medical advice, diagnosis, or treatment. Always seek the advice of a qualified healthcare provider for any questions or concerns you may have regarding a medical condition. Reliance does not endorse or recommend any specific tests, physicians, procedures, opinions, or other information mentioned on the blog.
Sucrose, glucose, and fructose are three common types of sugar that are absorbed differently and have different effects on the body.
Sucrose, glucose, and fructose are three types of sugar that contain the same number of calories gram for gram. They’re all found naturally in fruits, vegetables, dairy products, and grains but are also added to many processed foods.
They differ in their chemical structures, the way your body digests and metabolizes it different
Glucose
Glucose is a simple sugar, or monosaccharide. It’s your body’s preferred carb-based energy source Monosaccharides are made up of one single unit of sugar and thus cannot be broken down into simpler compounds.
It’s often added to processed foods in the form of dextrose, which is extracted from corn or wheat.
Glucose is less sweet than both fructose and sucrose (2).
Sucrose is the scientific name for table sugar.
Sugars are categorized as monosaccharides or disaccharides. Disaccharides are made up of two linked monosaccharides and are broken back down into monosaccharides during digestion
Sucrose is a disaccharide consisting of one glucose molecule and one fructose molecule, or 50% glucose and 50% fructose. sucrose, or table sugar, organic compound, colourless sweet-tasting crystals that dissolve in water. Sucrose (C12H22O11) is a disaccharide; hydrolysis, by the enzymeinvertase, yields “invert sugar” (so called because the hydrolysis results in an inversion of the rotation of plane polarized light), a 50:50 mixture of fructose and glucose, its two constituentmonosaccharides.
Sucrose occurs naturally in sugarcane, sugar beets, sugar maple sap, dates, and honey. It is produced commercially in large amounts (especially from sugarcane and sugar beets) and is used almost entirely as food. it’s also added to many processed foods, such as candy, ice cream, breakfast cereals, canned foods, soda, and other sweetened beverages.
\
Sucrose tastes less sweet than fructose alone but sweeter than glucose alone (2).
FructoseFructose, or “fruit sugar,” is a monosaccharide like glucose .
It’s naturally found in fruit, honey, agave, and most root vegetables. Moreover, it’s commonly added to processed foods in the form of high fructose corn syrup.
Fructose is sourced from sugar cane, sugar beets, and corn. High -fructose corn syrup is made from cornstarch and contains more fructose than glucose, compared with regular corn syrup (3Trusted Source).
Of the three sugars, fructose has the sweetest taste but the least impact on your blood sugar
SUMMARY
Sucrose is made up of the simple sugars glucose and fructose. Sucrose, glucose, and fructose are found naturally in many foods but are also added to processed products.
Your body digests and absorbs monosaccharides and disaccharides differently.
Since monosaccharides are already in their simplest form, they don’t need to be broken down before your body can use them. They’re absorbed directly into your bloodstream, primarily in your small intestine (5).
On the other hand, your body must break down disaccharides like sucrose into simple sugars before absorbing them.
Once the sugars are in their simplest form, they’re metabolized differently.
Glucose absorption and use
Glucose is absorbed directly across the lining of the small intestine into your bloodstream, which delivers it to your cells
It raises blood sugar more quickly than other sugars, which stimulates the release of insulin
Insulin is needed for glucose to enter your cells
Once inside your cells, glucose is either used immediately to create energy or turned into glycogen to be stored in your muscles or liver for future use
Your body tightly controls your blood sugar levels. When they get too low, glycogen is broken down into glucose and released into your blood to be used for energy
If glucose is unavailable, your liver can make this type of sugar from other fuel sources
Fructose absorption and use
Like glucose, fructose is absorbed directly into your bloodstream from the small intestine
It raises blood sugar levels more gradually than glucose and does not appear to immediately affect insulin levels
However, even though fructose doesn’t raise your blood sugar right away, it may have more long-term negative effects.
Your liver has to convert fructose into glucose before your body can use it for energy.
Eating large amounts of fructose on a high calorie diet can raise blood triglyceride levels
Excessive fructose intake may also raise the risk of metabolic syndrome and nonalcoholic fatty liver disease
Sucrose absorption and use
Enzymes in your mouth partially break down sucrose into glucose and fructose. However, the majority of sugar digestion happens in the small intestine (5).
The enzyme sucrase, which is made by the lining of your small intestine, splits sucrose into glucose and fructose. The glucose and fructose are then absorbed into your bloodstream as described above (15).
The presence of glucose increases the amount of fructose that is absorbed and also stimulates the release of insulin. Excessive absorption of fructose can promote the increased creation of fat stores in the liver
This means that eating fructose and glucose together may harm your health more than eating them separately (17).
It may explain why added sugars like high fructose corn syrup are linked to various health issues.
SUMMARY
Glucose and fructose are absorbed directly into your bloodstream, while sucrose must be broken down first. Glucose is used for energy or stored as glycogen. Fructose is converted to glucose or stored as fat.
Your body converts fructose to glucose in the liver to use it for energy. Excess fructose from processed foods and beverages places a burden on your liver, which may lead to a series of metabolic problems
Naturally derived fructose from fruit sources is not associated with the same negative health outcomes. Fruit does not contain the same combination of glucose and fructose that the widely used artificial ingredient high fructose corn syrup does.
Additionally, the health benefits of eating fruit outweigh any potential negative effects of its natural fructose, given the high fiber content and vitamins, minerals, and antioxidants found in fruit
Fruit should be eaten as part of a balanced diet that also consists of whole grains, vegetables, lean proteins, and healthy fats. The 2020–2025 Dietary Guidelines for Americans recommend that adults eat 2–2.5 servings of fruit daily (20Trusted Source).
Several studies have demonstrated the harmful effects of high fructose corn syrup. These include insulin resistance, type 2 diabetes, obesity, fatty liver disease, and metabolic syndrome (
In one 10-week study, people who drank fructose-sweetened beverages had an 8.6% increase in belly fat, compared to 4.8% in those who drank glucose-sweetened drinks
Another study found that while all added sugars can increase your risk of type 2 diabetes and obesity, high fructose corn syrup may be the most harmful
What’s more, fructose has been shown to increase the hunger hormone ghrelin and may make you feel less full after eating
Since fructose is metabolized in your liver like alcohol, some evidence suggests that it may be similarly addictive. One study found that it activates the reward pathway in your brain, which may lead to increased sugar cravings
SUMMARY
Fructose in processed foods and beverages has been linked to several negative health effects, including obesity, type 2 diabetes, insulin resistance, and fatty liver disease. Consuming fructose may also increase feelings of hunger and sugar cravings.
Fructose, the sweetest tasting carbohydrate (CHO), is consumed in significant amounts in the human diet. It occurs naturally in fresh fruits, vegetables and honey, with its traditional consumption ranging between 16 and 20 g/day. However, over the past 40 years, the intake of processed foods and beverages that are sweetened with High Fructose Corn Syrup (HFCS) or sucrose has escalated dramatically, resulting in significant increases in dietary fructose intake, to levels reaching as high as 85–100 g/day [1]. Temporal trend investigations have suggested parallel increasing trends in the prevalence of obesity, type 2 diabetes and cardiovascular diseases around the globe [2,3,4,5]. It was postulated that the metabolism of dietary fructose increases the risk of the metabolic syndrome (MetS) [2, 6], a constellation of cardiometabolic risk factors including insulin resistance, elevated blood pressure (BP), impaired glucose tolerance, hyperglycemia, atherogenic dyslipidemia (hypertriglyceridemia coupled with low high-density lipoprotein cholesterol (HDL-C) levels) and central adiposity [7, 8]. In turn, the MetS increases the risk for developing type 2 diabetes, cardiovascular diseases and all-cause mortality [9, 10]. A longitudinal study of 2902 adults followed for 11 years, showed that participants with the MetS had an adjusted relative risk for type 2 diabetes of 10.3 (5.44–19.5) and for cardiovascular diseases of 2.13 (1.43–3.18) [11].
Animal experiments and human clinical studies have investigated some of the mechanistic links between high fructose intake and the MetS, and suggested that excessive fructose intake may activate lipogenesis, induce insulin resistance and increase the risk of hypertension [12,13,14,15,16,17,18,19,20]. Fructose metabolism may also stimulate uric acid production leading to hyperuricemia [21], an independent risk factor for many pathological conditions, including the MetS [22]. However, in many instances, these studies have been criticized for using unrealistically high amounts of pure fructose [17, 23, 24]. Evidence from epidemiological studies that investigated current amounts of dietary fructose consumption and their association with the MetS are scarce and have produced controversial findings [25,26,27,28]. Indeed, an analysis of the National Health and Nutrition Examination Survey (NHANES) 1999–2006 database indicated that fructose ordinary consumption in the American diet was not positively associated with indicators of MetS [25]. On the other hand, other epidemiological studies have indicated a positive association of fructose consumption with cardiometabolic abnormalities [27, 28]. In some other studies, the association between fructose intake and cardiometabolic risk factors lost significance when the analysis was adjusted for body weight [29], suggesting that obesity may be responsible for the development of these cardiometabolic factors rather than fructose intake. For instance, an analysis of healthy male adults (n = 40,389) from the longitudinal Health Professionals Follow-Up Study, showed that the significant association between sugar-sweetened beverage (SSB) consumption and type 2 diabetes lost its significance after adjustment for confounders, which included body mass index (BMI) [29, 30]. The discrepancy in findings may also result from the fact that many of the available epidemiological studies have assessed the association between MetS and total fructose intake, without any differentiation between naturally occurring vs. added fructose intakes. Dietary sources of naturally occurring fructose include fruits and vegetables that are rich in antioxidants, phytochemicals, fiber, minerals and vitamins, and which are individually and synergistically beneficial to cardiometabolic health [1, 25]. In contrast, the sources of added fructose are mostly high sugar, energy-dense processed foods that were linked to increased cardiometabolic risk [1, 14, 25].
The controversy in the available findings highlights the need for more research examining dietary fructose intake as a cardiometabolic risk factor in epidemiological settings, while also distinguishing between naturally occurring vs. added fructose intakes. To date, the association between dietary fructose and the MetS has not been investigated in the Arab Eastern Mediterranean Region (EMR), a region that is witnessing the nutrition transition with its characteristic shifts in diet, lifestyle and body composition [31]. The region harbors one of the highest rates of obesity and the MetS worldwide [32], while also witnessing significant increases in sugar intakes [33]. Lebanon, a small country of the EMR, is no exception with earlier studies reporting a high prevalence of the MetS (34.7%) [34] in the adult population, while data on dietary fructose intake are completely lacking. It is in this context that this study was conducted with the aim of (1) assessing total dietary fructose intake in a sample of Lebanese healthy adults, and determining the intake levels of natural vs. added fructose; (2) investigating the association of dietary fructose with the MetS in the study population; and (3) identifying the socioeconomic and lifestyle factors associated with high fructose intake.
There is no need to avoid sugars that are naturally found in whole foods, such as fruits, vegetables, and dairy products. These foods also contain nutrients, fiber, and water, which counter any of their negative effects.
The harmful health effects associated with sugar consumption are due to the high amount of added sugar in the typical Western diet.
A survey of over 30,000 Americans found that the average person consumed 68 grams of added sugars per day, or approximately 13% of their total calories — far more than the daily recommendation
The World Health Organization (WHO) recommends limiting added sugars to 5–10% of your daily calorie consumption. In other words, if you’re eating 2,000 calories per day, keep added sugars to less than 25–50 grams .
To put that into perspective, one 12-ounce (355 ml) can of soda contains nearly 40 grams of added sugar, which is enough to push you over your daily limit
Sugars are not only added to foods that are obviously sweet like sodas, ice cream, and candy. They are also added to foods you wouldn’t necessarily expect, such as condiments, sauces, and frozen foods.
When buying processed foods, always read the ingredient list carefully to look for hidden sugars. Keep in mind that sugar can be listed by over 50 different names.
The most effective way to reduce your sugar intake is to eat mostly whole and unprocessed foods.
SUMMARY
Added sugars should be limited, but there is no need to worry about those found naturally in foods. Consuming a diet high in whole foods and low in processed foods is the best way to avoid added sugars.
Glucose and fructose are simple sugars, or monosaccharides.
Your body can absorb them more easily than the disaccharide sucrose, which must be broken down first.
Added fructose may have the most negative health effects, but experts agree that you should limit your intake of all types of added sugar.
However, there is no need to limit the sugars found naturally in fruits and vegetables.
To ensure a healthy diet, eat whole foods whenever possible and save added sugars for the occasional special
Fructose, the sweetest tasting carbohydrate (CHO), is consumed in significant amounts in the human diet. It occurs naturally in fresh fruits, vegetables and honey, with its traditional consumption ranging between 16 and 20 g/day. However, over the past 40 years, the intake of processed foods and beverages that are sweetened with High Fructose Corn Syrup (HFCS) or sucrose has escalated dramatically, resulting in significant increases in dietary fructose intake, to levels reaching as high as 85–100 g/day [1]. Temporal trend investigations have suggested parallel increasing trends in the prevalence of obesity, type 2 diabetes and cardiovascular diseases around the globe [2,3,4,5]. It was postulated that the metabolism of dietary fructose increases the risk of the metabolic syndrome (MetS) [2, 6], a constellation of cardiometabolic risk factors including insulin resistance, elevated blood pressure (BP), impaired glucose tolerance, hyperglycemia, atherogenic dyslipidemia (hypertriglyceridemia coupled with low high-density lipoprotein cholesterol (HDL-C) levels) and central adiposity [7, 8]. In turn, the MetS increases the risk for developing type 2 diabetes, cardiovascular diseases and all-cause mortality [9, 10]. A longitudinal study of 2902 adults followed for 11 years, showed that participants with the MetS had an adjusted relative risk for type 2 diabetes of 10.3 (5.44–19.5) and for cardiovascular diseases of 2.13 (1.43–3.18) [11].
Animal experiments and human clinical studies have investigated some of the mechanistic links between high fructose intake and the MetS, and suggested that excessive fructose intake may activate lipogenesis, induce insulin resistance and increase the risk of hypertension [12,13,14,15,16,17,18,19,20]. Fructose metabolism may also stimulate uric acid production leading to hyperuricemia [21], an independent risk factor for many pathological conditions, including the MetS [22]. However, in many instances, these studies have been criticized for using unrealistically high amounts of pure fructose [17, 23, 24]. Evidence from epidemiological studies that investigated current amounts of dietary fructose consumption and their association with the MetS are scarce and have produced controversial findings [25,26,27,28]. Indeed, an analysis of the National Health and Nutrition Examination Survey (NHANES) 1999–2006 database indicated that fructose ordinary consumption in the American diet was not positively associated with indicators of MetS [25]. On the other hand, other epidemiological studies have indicated a positive association of fructose consumption with cardiometabolic abnormalities [27, 28]. In some other studies, the association between fructose intake and cardiometabolic risk factors lost significance when the analysis was adjusted for body weight [29], suggesting that obesity may be responsible for the development of these cardiometabolic factors rather than fructose intake. For instance, an analysis of healthy male adults (n = 40,389) from the longitudinal Health Professionals Follow-Up Study, showed that the significant association between sugar-sweetened beverage (SSB) consumption and type 2 diabetes lost its significance after adjustment for confounders, which included body mass index (BMI) [29, 30]. The discrepancy in findings may also result from the fact that many of the available epidemiological studies have assessed the association between MetS and total fructose intake, without any differentiation between naturally occurring vs. added fructose intakes. Dietary sources of naturally occurring fructose include fruits and vegetables that are rich in antioxidants, phytochemicals, fiber, minerals and vitamins, and which are individually and synergistically beneficial to cardiometabolic health [1, 25]. In contrast, the sources of added fructose are mostly high sugar, energy-dense processed foods that were linked to increased cardiometabolic risk [1, 14, 25].
The controversy in the available findings highlights the need for more research examining dietary fructose intake as a cardiometabolic risk factor in epidemiological settings, while also distinguishing between naturally occurring vs. added fructose intakes. To date, the association between dietary fructose and the MetS has not been investigated in the Arab Eastern Mediterranean Region (EMR), a region that is witnessing the nutrition transition with its characteristic shifts in diet, lifestyle and body composition [31]. The region harbors one of the highest rates of obesity and the MetS worldwide [32], while also witnessing significant increases in sugar intakes [33]. Lebanon, a small country of the EMR, is no exception with earlier studies reporting a high prevalence of the MetS (34.7%) [34] in the adult population, while data on dietary fructose intake are completely lacking. It is in this context that this study was conducted with the aim of (1) assessing total dietary fructose intake in a sample of Lebanese healthy adults, and determining the intake levels of natural vs. added fructose; (2) investigating the association of dietary fructose with the MetS in the study population; and (3) identifying the socioeconomic and lifestyle factors associated with high fructose intake.
Allulose: What to Know About This Sugar Alternative
3 min read
What Is Allulose?
Allulose is a rare sugar that naturally occurs in fruits like figs and raisins. “It’s about 70% as sweet as sugar,” s
Basic sugar (called sucrose) is the most well-known form of sweetener. But there are many other types of sugar that are in or added to foods. There are simple sugars, called monosaccharides, which contain a single sugar molecule. These include glucose, fructose, galactose, ribose, and xylose. And then there are disaccharides, which are two sugar molecules bonded together, like sucrose, lactose, and maltose.
Allulose is a monosaccharide. It has 90% fewer calories than sucrose, which makes it virtually calorie-free. Researchers have recently found ways to produce allulose on a larger scale, which may allow it to become a popular sweetener in the future.
Is Allulose Healthy?
The FDA states that allulose is “generally recognized as safe” (GRAS).
“Basically, they know that small amounts aren’t going to do any harm to people if they consume it,” DiMarino says. “What I recommend with my patients is that whatever you’re using, whether it’s natural sugar … or any artificial sweetener, is that you use your best judgment and use it in small amounts in moderation. Because we don’t want to rely on them too much.”
If you follow these suggestions, allulose can be a great replacement to regular sugar.
“What’s interesting is that it’s not metabolized by the body. It’s absorbed by the small intestine, but then actually excreted. So none of the calories get absorbed or stored in your body,” DiMarino says. “With the limited research that’s been done, it’s been found that [allulose] doesn’t have effects on blood sugars or an insulin response.”
Most people who eat allulose in moderation won’t notice any major issues. But it’s important to note that everyone has a different tolerance to artificial sweeteners. “One side effect that people tend to see is some gastrointestinal discomfort, like maybe some bloating, or some issues going to the bathroom,” DiMarino says.
For that reason, it’s a good idea to add small amounts of allulose to your food at first.
“It’s more so trial and error in finding how much is your limit,” DiMarino says. “But if you eat it in small amounts over the period of the day, or just sparingly throughout the week, you shouldn’t end up having any kind of side effects.”
Who Should Use Allulose?
Allulose can be a good substitute if you want to cut back on the amount of sugar or overall calories you eat. You can use it to make baked goods, frozen desserts, or your favorite drink.
Since the sweetener has an extremely low sugar content, people on the ketogenic or “keto” diet have started to use allulose more. People who are on the keto diet eat very few carbohydrates. Allulose doesn’t have many, so it may be a good choice for keto-friendly sweets.
Allulose also doesn’t affect your blood sugar or insulin levels. So it may be agood alternative for people with certain conditions like diabetes.
“The two groups of people I feel like this would be most beneficial for would be people with diabetes, especially those who are trying to reduce their blood sugar. And people who are overweight or obese and trying to cut back on calories,” DiMarino says.
Who Shouldn’t Eat Allulose?
If you’re allergic to any artificial or alternative sweetener, you should stay away from allulose. But allergies to these sweeteners aren’t very common.
Experts are still studying how constant use of artificial or alternative sweeteners affect humans.
Some studies have linked the use of certain sugar substitutes with an increased risk for cancer and/or obesity. Most of these studies have been done on animals. It’s not known if they would have the same effect on people.
Most importantly, DiMarino suggests eating a balanced diet.
“Try and eat whole, high-quality foods that are minimally processed and that are lower in sugar. Use these alternatives and these sugar alcohols sparingly, in moderation,” DiMarino says
Exposure to lead through sources such as contaminated food, soil, and paint might have contributed to 5.5 million adult cardiovascular disease deaths and 765 million lost IQ points among children younger than 5 years in 2019, according to a new analysis of countries’ blood lead level estimates.
Low- and middle-income countries combined bore up to 95% of the losses. Moreover, the estimated IQ loss and deaths from cardiovascular disease were about 80% higher and 6 times greater, respectively, than earlier approximations for low- and middle-income countries.
The results suggest that the magnitude of environmental risk from lead exposure is similar to that of fine-particulate air pollution and exceeds the risks associated with unsafe household drinking water, sanitation, and handwashing, the researchers reported in The Lancet Planetary Health.
Antibiotics ‘Like Gold’ for Some, Driving Inappropriate Use
October 16, 2023
1
Personal beliefs and healthcare system barriers contribute to inappropriate antibiotic use by patients, report researchers presenting results at the IDWeek 2023 Annual Meeting.
Nonprescription antibiotic use includes accessing medication left over from a prior prescribed course, obtained from social networks, and purchased over-the-counter in other countries or illegally in stores and markets in the United States.
Overuse and misuse of antibiotics contributes to a growing threat of antimicrobial resistance, and it is tough to say how common it is, Lindsey A. Laytner, PhD, MPH, with Baylor College of Medicine in Houston, Texas, pointed out in her presentation.
“This is an understudied area. We don’t routinely collect these data, so we don’t actually know what the true prevalence is. The factors that contribute to this unsafe practice in the US are also underexplored,” Laytner said.
To investigate, the researchers conducted in-depth interviews with 86 adults (median age, 49 years; 62% women) to identify patients’ motivations to use antibiotics without a prescription. All of them answered “yes” when asked in a previous survey whether they would use antibiotics without contacting a doctor, nurse, dentist, or clinic.
Laytner said several prominent themes emerged.
Nearly all interviewees reported nonprescription antibiotic use for symptoms that mostly do not warrant antibiotics. These included symptoms of COVID-19, influenza, and the common cold, as well as for pain management, allergies, and even wounds.
Ineffectively Treating Symptoms
Many felt they “knew their body, knew what they had, and knew how to treat themselves” without a healthcare provider, Laytner said.
They also felt the over-the-counter medicines “don’t always work and that antibiotics are like gold or this cure-all and because they are difficult to get a prescription for, they should be kept on hand,” she explained.
A variety of healthcare system barriers also contribute to inappropriate antibiotic use, including long wait times to schedule appointments and to see the doctor while at their appointments; high costs for clinic visits and prescriptions; and transportation issues.
Many patients opted to use nonprescription antibiotics out of “convenience,” Laytner added.
She explains that the findings could help inform community-level education efforts on inappropriate use of antibiotics and help shape policies to promote antibiotic stewardship.
IDWeek 2023 Annual Meeting: Abstract 1016. Presented October 12, 2023.
Vegans follow a plant-based diet and avoid all animal-based foods such as meat, poultry, fish, shellfish, dairy, eggs, and honey. Many also refrain from buying animal-derived products (e.g., leather and reptile skin). Generally, veganism disavows anything involving animal exploitation, including the use of animals for entertainment and product testing.
However Veganism is unhealthy when you’re not getting all the proper nutrients. Adopting a vegan diet needs initial planning with a dietitian and also if you are of a childbearing age, it is more important to plan your diet for dietary supplements
Animal-derived ingredients like gelatin, albumin, casein, carmine, and pepsin can be found in marshmallows, gummy candies, chewing gum, etc. Vegans must diligently check food labels when grocery shopping.
Although eating a vegan diet may seem limiting, there are far more plant-based options on the market today. Vegans enjoy fruits and vegetables, legumes (like beans and lentils), grains and seeds, nuts and nut butters, plant-based milks, and soy products such as tofu.
Plant-based meats and cheeses have also become readily available, but it’s best to consume mostly fresh produce and whole grains rather than mass-produced, processed items. Uncontrolled eating of unhealthy carbohydrates can occasionally cause weight gain
Health benefits of veganism
When it’s well-planned and executed, the health benefits of veganism are numerous. Since this diet relies heavily on fresh fruits and vegetables, nuts, seeds, whole grains, and legumes, it’s usually rich in nutrients.
Whole foods contain tons of vitamins, minerals, antioxidants, and fiber, while being low in saturated fats and cholesterol. A well-rounded vegan diet supplies vitamins B1, C, and E, as well as fiber, magnesium, folic acid, and iron. Just remember to incorporate proteins and essential amino acids, which ordinarily come from animal-based sources.
As with any lifestyle, certain pros and cons of veganism should be considered. However, the wide array of health benefits includes:
Improved blood sugar control: Unfortunately, type 2 diabetes is becoming more prevalent in the U.S. But vegetarian and vegan lifestyles present potential advantages for the management of this chronic condition. In clinical trials, individuals increased glycemic control to a greater extent with low-fat vegan diets than with conventional diabetes diets. In observational studies, individuals on vegetarian diets prove roughly half as likely to develop diabetes, compared to non-vegetarians.
Weight loss: Since they contain more fat and calories than plant-based foods, eliminating meat, dairy, and other animal products can help you lose weight and lower cholesterol. According to the American Journal of Clinical Nutrition, vegans tend to have lower body weight and reduced blood pressure.
Decreased chance of cardiovascular and heart disease: Certain contributing factors for heart disease depend on your daily diet. Lower cholesterol, blood pressure, and glucose levels keep your heart in tip-top shape. Generally speaking, vegans are more likely to consume heart-healthy foods including nuts, whole grains, and vegetables.
Decreased chance of developing certain cancers: Eating too much meat, especially processed varieties (e.g., hot dogs, deli meat) may make you more susceptible to colon and esophageal cancer, among other problems. However, vegan diets (known for being high in fiber) could help improve your odds for avoiding those issues.
Negative effects of veganism
The transition to a plant-based lifestyle should be well-planned in order to avoid the dangers of a vegan diet. Potentially serious nutritional deficiencies and vegan health risks must be taken into account. See your doctor or nutritionist to ensure you don’t miss out on proteins and other key nutrients only found in meat, dairy, and eggs.
Going vegan side effects sometimes include anemia, disruptions in hormone production, vitamin B12 deficiencies, and deficiency of omega 3 fatty acids . That’s why it’s crucial to include plenty of vitamin B12, vitamin D, iron, calcium, iodine, zinc, and omega-3s in your diet.
ONE of the main concerns is vitamin B12 deficiencies in food and you do neeed take vit B12. supplementsor foods supplemented with vitamin D
Some of these nutrients are added to fortified cereals, plant milks, tofu, and nutritional yeast. Legumes and dark, leafy vegetables provide iron and calcium, while tofu is a great source of protein, calcium, and zinc. Lastly, omega-3s, such as DHA and ALA, can be found in walnuts, canola oil, soy products, and ground flaxseed.
What are some other cons of veganism? Believe it or not, weight gain is one reason why being vegan is bad fora few people. It’s often the result of eating too much processed junk food, which is high in fat and calories. Switching to a plant-based diet may leave you feeling hungry. Opt instead for whole grains, lean proteins, and other foods that keep you feeling fuller longer.
It is very important to talk to your doctor about veganism pros and cons. Determine whether you need daily supplements, or have any conditions which may lead to problems with a vegan diet. Then be sure to follow up with routine visits and blood tests.
FROM THE VEGAN SOCIETY -UK
“Veganism is a philosophy and way of living which seeks to exclude—as far as is possible and practicable—all forms of exploitation of, and cruelty to, animals for food, clothing or any other purpose; and by extension, promotes the development and use of animal-free alternatives for the benefit of animals, humans and the environment. In dietary terms it denotes the practice of dispensing with all products derived wholly or partly from animals.”
There are many ways to embrace vegan living. Yet one thing all vegans have in common is a plant-based diet avoiding all animal foods such as meat (including fish, shellfish and insects), dairy, eggs and honey – as well as avoiding animal-derived materials, products tested on animals and places that use animals for entertainment.
Some people may choose to go vegan, for some it may be because they do not believe in farmed animal practices and animal exploitation, for others it may be due to environmental concerns. Whatever the reason The Vegan Society is here to support everyone on their vegan journey.
History
Although the vegan diet was defined early on in The Vegan Society’s beginnings in 1944, by Donald Watson and our founding members.It was as late as 1949 before Leslie J Cross pointed out that the society lacked a definition of veganism. He suggested “[t]he principle of the emancipation of animals from exploitation by man”. This is later clarified as “to seek an end to the use of animals by man for food, commodities, work, hunting, vivisection, and by all other uses involving exploitation of animal life by man”.
The society was first registered as a charity in August 1964 but its assets were later transferred to a new charity when it also became a limited company in December 1979. The definition of veganism and the charitable objects of the society were amended and refined over the years. By winter 1988 the current definition was in use – although the phrasing has changed slightly over the years.
A great deal – you’ll soon find a whole new world of exciting foods and flavours opening up to you. A vegan diet is richly diverse and comprises all kinds of fruits, vegetables, nuts, grains, seeds, beans and pulses – all of which can be prepared in endless combinations that will ensure you’re never bored. From curry to cake, pasties to pizzas, all your favourite things can be suitable for a vegan diet if they’re made with plant-based ingredients. Check out our vegan recipes for ideas.
It’s not just about diet
Vegans avoid exploiting animals for any purpose, with compassion being a key reason many choose a vegan lifestyle. From accessories and clothing to makeup and bathroom items, animal products and products tested on animals are found in more places than you might expect. Fortunately nowadays there are affordable and easily-sourced alternatives to just about everything. With over 65,000 products and services registered with our Vegan Trademark alone, living a vegan lifestyle has never been easier. Browse our online shop today.
Start your vegan journey today by downloading our VeGuide app. You can also join The Vegan Society by completing our quick and simple online form. As a registered charity we rely on our members, and we are so grateful to everyone who supports us. For just £2 a month, your membership will go towards helping us to spread the word of veganism and create a world where animals are free to exist in their own right. In return you’ll receive access to over one hundred vegan discounts, our quarterly magazine, exclusive competitions and more!
Other aspects of vegan living
Medicine
Currently all medicine in the UK must be tested on animals before it is deemed safe for human use, but please note: The Vegan Society DOES NOT recommend you avoid medication prescribed to you by your doctor – a vegan who is looking after themselves the best they can is an asset to the movement. What you can do is ask your GP or pharmacist to provide you, if possible, with medication that does not contain animal products such as gelatine or lactose. For more information visit the medicines website, which contains information on medicines prescribed in the UK, including ingredients lists.
Medical charities
If you’re a medical charity supporter you may wish to check whether your chosen charity performs animal testing. There are many charities that don’t currently conduct animal tests and many vegans prefer donating to charities that actively seek alternative methods of testing.
Entertainment
Vegans choose not to support animal exploitation in any form and so avoid visiting zoos or aquariums, or taking part in dog or horse racing. A great alternative is visiting and supporting animal sanctuaries that provide safe and loving homes for rescued animals.
Want to find out more about the vegan lifestyle? Sign up to the free Vegan Pledge today. There are hundreds of thousands of vegans across the globe – with you, we’re that much stronger.
Go Vegan
Sign-up for our newsletter
Join our newsletter to receive monthly competitions, offers and information on all things vegan.
Among women with genitourinary syndrome of menopause, 12 weeks of treatment with vaginal suppositories containing hyaluronic acid (HLA) reduces vulvovaginal symptoms, according to trial results presented at the 2023 Menopause Meeting. HLA may be a promising nonhormonal therapy for this condition, the researchers said.
METHODOLOGY:
Investigators randomly assigned 49 women to receive treatment with a vaginal suppository containing 5 mg of HLA or standard-of-care treatment with vaginal estrogen cream (0.01%).
The trial was conducted between September 2021 and August 2022.
The VSQ assesses vulvovaginal symptoms associated with menopause such as itching, burning, and dryness, as well as the emotional toll of symptoms and their effect on sexual activity.
Change in VSQ score did not significantly differ between the treatment groups. The measure improved from 5.2 to 1.7 in the group that received estrogen, and from 5.8 to 2.5 in those who received HLA (P = .81).
No treatment-related severe adverse events were reported.
“
SOURCE:
Poster P-1 was presented at the 2023 meeting of the Menopause Society, held September 27-30 in Philadelphia.
DISCLOSURES:
The study was funded by Bonafide Health, a company that sells supplements to treat menopause symptoms, including vaginal suppositories containing HLA.
DIETARY PATTERNS, FOODS, AND NUTRIENTS TO AMELIORATE NON-ALCOHOLIC FATTY LIVER DISEASE: A SCOPING REVIEW
ABSTRACT
Background: Non-alcoholic fatty liver disease (NAFLD) is the most common cause of chronic liver disease without pharmacological treatment
yet. There is also a lack of specific dietary recommendations and strategies to treat the negative health impacts derived from NAFLD.
Objective: This scoping review aimed to compile dietary patterns, foods, and nutrients to ameliorate NAFLD.
Methods: A literature search was performed through MEDLINE, Scopus, Web of Science, and Google Scholar. Results: Several guidelines are available through the literature. Hypocaloric Mediterranean diet is the most accepted dietary pattern to tackle NAFLD. Coffee consumption (sugar free) may have a protective effect for NAFLD. Microbiota also plays a role in NAFLD; hence, fibre intake should be guaranteed. Conclusions: A high-quality diet could improve liver steatosis. Weight loss through hypocaloric diet together with physical activity and limited sugar intake are good strategies for managing NAFLD. Specific dietary recommendations and a Mediterranean plate have been proposed to ameliorate NAFLD.
The most usual cause of chronic liver disease worldwide is non-alcoholic fatty liver disease (NAFLD), with a worldwide prevalence of 20–30% of the adult population worldwide in 2017 [1], and an overall prevalence of 32.4% in 2022, which continues rising globally [2]. Non-alcoholic steatohepatitis (NASH) is the major contributor to the advancement of cirrhosis and hepatocellular carcinoma [3,4], which is the second most important cause of lost life years among all cancers [5].
NAFLD causes ongoing medical expenses, financial losses, and a decline in the quality of life [6,7,8]. It is also associated with obesity, metabolic syndrome (MetS) [9], type 2 diabetes mellitus (T2DM) [10], cardiovascular diseases (CVD) [11], hypertension, and chronic kidney disease (CKD) [12]. A proportion of cases has a normal body mass index (BMI), which is known as “non-obese NAFLD” or “lean NAFLD” [13]. Worldwide prevalence of non-obese NAFLD is growing substantially [14]. Lean NAFLD subjects showed similar complications and comorbidities to their obese counterparts, such as T2DM, cardiovascular diseases, and hepatocellular carcinoma [15,16]. Then, NAFLD is a major threat globally.
The recommended NAFLD/NASH treatment is changes in lifestyle (i.e., increasing exercise) [17]. Even in the absence of obesity, poor nutritional composition may put a person at risk for NAFLD [18,19]. The significance of weight loss (WL) is emphasized in these therapies, with a goal of a 7–10% decrease in body weight (BW) obtained by a hypocaloric diet (deficit of 500–1000 kcal/d) and/or physical activity. However, precise nutritional advice is inconsistent, and weight loss and maintenance remain a significant challenge for many people. The Mediterranean diet (MedDiet) is notably mentioned by the joint action of the European Association for the Study of the Liver (EASL)–the European Association for the Study of Diabetes (EASD)–the European Association for the Study of Obesity (EASO), by the European Society for Clinical Nutrition and Metabolism (ESPEN), and by the Asian Pacific Association for the Study of the Liver (APASL) as being advantageous for NAFLD patients [17,20,21,22]. Modifying dietary composition, with or without calorie restriction, may be a useful and long-lasting method of managing NAFLD [23,24]. The macronutrient proportion of the diet, particularly high intakes of carbohydrates, simple sugars, fats, proteins, and low fibre intake may be linked to the NAFLD risk, independent of excessive energy intake. The intake of certain nutrients may influence this disease, but its mechanism is not absolutely understood yet [23].
The aim of this scoping review is to compile dietary patterns, foods, and nutrients to ameliorate NAFLD.
2. Review Methodology
The relevant information on dietary treatment, weight loss strategies and dietary guidelines to ameliorate NAFLD was obtained from a literature search conducted between January and July 2023 through MEDLINE (via PubMed), Scopus, Web of Science and Google Scholar. MeSH terms used for the search were “non-alcoholic fatty liver disease”, “diet/dietary treatment”, “dietary guideline”, “weight loss strategy”. The most relevant data were summarized, and the results are presented in the following sections. Only papers written in English and Spanish were considered. A publication date filter was not applied, as the study of dietary treatment for NAFLD is quite recent.
3. Current Dietary Guidelines
Dietary guidelines are an important tool to address NAFLD based on a target population; however, they are unspecific regarding dietary recommendations for NAFLD patients. Scientific associations [17,20,21,22] highlighted the importance of weight loss targeting 7–10% reduction in body weight achieved by hypocaloric diets (energy deficit of 500–1000 kcal/day) and/or physical activity to promote a caloric deficit. EASL–EASD–EASO and APASL recommended the exclusion of processed food and added fructose. There is low evidence supporting dietary composition. There are no recommendations for macronutrients, but the join action of the European Association for the Study of the Liver (EASL)–the European Association for the Study of Diabetes (EASD)–the European Association for the Study of Obesity (EASO), the European Society for Clinical Nutrition and Metabolism (ESPEN), and the Asian Pacific Association for the Study of the Liver (APASL) mentioned that the MedDiet is useful to reduce liver fat and improve NAFLD. Table 1 shows the guidelines from the scientific associations that were made for different target populations.
Table 1. Recommendations of scientific associations on dietary guidelines for NAFLD.
4. Diet Impact in NAFLD, Gut Microbiota, and Macronutrients
Independently of weight loss and energy intake, a healthy diet is effective in decreasing the liver fat contents and thus protecting the liver from cardiometabolic morbidity and mortality [24].
Research showed that foods considered to be beneficial to prevent and avoid progression of NAFLD are fruits and vegetables, whole grain cereals, fatty fish (mainly rich in omega 3), and extra virgin olive oil [25]. It was pointed out that there is evidence that detrimental dietary composition predisposes an individual to NAFLD, even without obesity [19].
The foods considered NAFLD promoters are red meat and processed meats, soda, processed foods, cakes, and biscuits [24]. Diet directly impacts the process of de novo lipogenesis, in which hepatocytes transform the excess of carbohydrates, especially fructose, into fatty acids [26].
Daily intake of fructose is linked to high fibrosis, which is mainly due to industrial fructose and not to fruit-derived fructose [27]. This effect could be mediated by hepatic ATP depletion.28].
A cross-sectional study found that high consumption of red and/or processed meat was related to insulin resistance and NAFLD [29]. High animal protein intake was related to NAFLD in overweight patients [30]. Diet promotes NASH by modulating hepatic triglyceride accumulation and antioxidant activity by means of changes in postprandial triglyceride metabolism and insulin sensitivity [18,31].
Diet may prevent or trigger liver lipid accumulation by influencing the relationship between liver, adipose tissue, and gut, regardless of energy intake. For instance, formulations of high-fructose diets induced distinct changes in intestine microbiota. It has been reported that a high-fructose corn syrup reduced butyrate-producing bacteria and the Firmicutes/Bacteroidetes ratio linked to the metabolic syndrome pathogenesis [32,33], but high-fructose diet from fruits induced an opposite shift [34].
The macronutrient composition was related to NAFLD/NASH development [35]. Regarding carbohydrates, it was established that fructose is the primary carbohydrate determinant in hepatic fat formation. Fructose has a detrimental metabolic impact promoting de novo lipogenesis (DNL) and liver fat storage [36]. For instance, the MedDiet is characterized by low carbohydrate intake (low-fat diet: 40% calories vs. 50–60%), with low sugars and refined carbohydrates [37]. According to a previous study, 15% of liver fat is obtained from diet, and this percentage may rise if dietary fat consumption exceeds 30% of daily energy needs [38]. Saturated fatty acids impair phospholipid metabolism and increase insulin resistance by promoting mitochondrial dysfunction, which modifies respiratory chain activity and ATP homeostasis, increases reactive oxygen species (ROS) synthesis, and induces apoptosis [39]. The literature shows controversial and scarce data on the dietary protein effects in NAFLD patients. Animal models suggest that dietary proteins have benefits for glucose metabolism. In population studies, animal protein-rich diets are linked to an increased risk of NAFLD development, especially in patients who are overweight [40]. Another risk factor for the severity of NAFLD is the presence of sarcopenia and obesity and insulin resistance and inflammation, which are increased in the coexistence of fat accumulation and muscle loss, leading to atherosclerotic damage and severe liver disease (NASH and advanced fibrosis) [41].
5. Nutrition, Genetics, and NAFLD
Diet even impacts the DNA homeostasis where calcium, folate, nicotinic acid, vitamin E, and retinol are cofactors of essential enzymes in the DNA synthesis and repair [42], whereas others such as the trans fatty acids induce DNA damage [43]. In NAFLD, telomeres shortening is typical [44], but vegetables, fibre, and omega-3 fatty acids prevent it, which was significantly associated with decreases in low-density lipoprotein (LDL) cholesterol and psychological distress, as well as the anti-inflammatory contents of the diet [45], suggesting the role of these factors in telomere biology maintenance and potentially impacting overall health status. Saturated fatty acids, processed meat, and carbohydrates with a high glycaemic index favour it [46,47].
A major determinant of liver fat contents and the NAFLD progression is the patatin-like phospholipase domain-containing 3 (PNPLA3). It increases a mutated protein with impaired lipase activity on hepatocyte lipid droplets, favouring the accumulation of triglycerides in the liver [48,49]. Acquired variables such as diet, and especially carbohydrate-rich diets, can cause the protein encoding by the mutant gene [50]. It is also influenced by fatty acids, particularly n-6/n-3 PUFA [51]. Another important genetic determinant is the variant of the transmembrane 6 superfamily member 2 gene (TM6SF2), which predisposes an individual to increase liver fat content due to the retention of lipids and the impairment in the liver the release of very low-density lipoprotein (VLDL) [52]. In comparison to the wild types, carriers of the mutant TM6SF2 allele improved fasting and postprandial lipid profiles, which decrease circulating atherogenic lipoproteins even after a high fat challenge [53]. It is suggested that diet may modulate the epigenetic modifications, affecting the liver lipid metabolism, mitochondrial function, oxidative stress, and insulin resistance [54,55]. DNA methylation is considered a crucial step in the development of NASH and the metabolism of triglycerides, and it may be increased by dietary deficiencies in choline, betaine, B12, and folate, where the deficiencies encourage the overexpression of genes involved in the fatty acid production, which in turn promotes the synthesis of hepatic triglycerides [56].
6. Western Diet vs. Mediterranean Diet
A dietary pattern represents the overall combination of foods usually consumed, together with effects on health [57]. Studies showed that people following a high-fat Western dietary pattern were at an increased risk of developing NAFLD and its severity, while people following a MedDiet were associated with amelioration in hepatic steatosis and a lower rate of NAFLD [57,58,59]. The Western diet has a strong positive association with weight gain, insulin resistance, and NAFLD [59,60,61]. The NAFLD level found in Australian adolescents was prospectively linked to the Western dietary pattern, independently of family income, physical activity, and sedentary behaviour [62]. This dietary pattern lacks a precise definition; nevertheless, it can be generally characterized by densely caloric food, high animal protein, low fruit and vegetable contents, overeating [63], refined grains, red and processed meats, and soft drinks [64]. Recent studies showed the relation between higher intake of red and processed meats and NAFLD [30,65,66,67]. When they were consumed in excess, even for a short time such as one week, diets high in SFAs and high in fructose increased hepatic steatosis [68]. Lifestyle linked to Western diets included physical inactivity, usual snacking, high chronic psychological stress, smoking, environmental pollution, insufficient sleep, and avoidance of sun exposure [69,70]. NAFLD is related to short sleep duration, poor sleep quality [71], together with a trend for obstructive sleep apnoea syndrome [72]. A recent study in China in around 90,000 adults found that long-term exposure to environmental air pollution may increase the risk of MAFLD, particularly in men, smokers, alcohol drinkers, people who eat high-fat diets, and people who have central obesity. A study with rats showed that chronic exposure to ultraviolet radiation may be a good complementary therapy in the development of NAFLD [73].
On the contrary, the MedDiet is a plant-rich food diet, with olive oil being the highest source of added fats, high or moderate consumption of fish and shellfish, moderate consumption of eggs, poultry, and dairy products (mainly as cheese and yogurt), low consumption of meat, and moderate intake of alcohol (mainly wine with meals). This diet is rich in monounsaturated fatty acids (MUFAs) mainly from olive oil and olives, includes low-fat dairy products, and encourages low consumption of red meat. It has proven benefits to prevent cardiovascular diseases, hypertension, hypercholesterolemia, and obesity [24,74]. Several dietary approaches could be used to treat NAFLD [75], but the MedDiet was found especially helpful to improve the NAFLD. Cross-sectional, longitudinal studies and clinical trials showed a lower probability of NASH in patients who adhered to the MedDiet [76,77,78]. A 6-month nutritional counselling study showed that adherence to the MedDiet was effective in improving disease-specific traits, including liver imaging, liver fibrosis score, inflammatory/oxidative biomarkers, and indices of glycaemic status in nonfibrotic NAFLD patients [23]. A clinical trial conducted in Spain among NAFLD and MetS patients showed that an increase in MedDiet adherence over 6 months was related to better outcomes in terms of body weight, waist circumference, and BMI, but also in blood pressure (both systolic and diastolic), and to a decrease in intrahepatic fat content. In other words, an increase in MedDiet adherence ameliorated intrahepatic fat content after 6 months of treatment [76]. The MedDiet has been shown to reduce liver fat and to improve hepatic insulin sensitivity independent of exercise and weight loss [77]. High adherence to the MedDiet was highly associated with low insulin resistance level, alanine aminotransferase (ALT), and NAFLD severity [17]. Similarly, high adherence to the MedDiet was found to be associated with low likelihood of high-grade steatosis and the presence of steatohepatitis [78]. The positive effect of the MedDiet on liver inflammation and fibrosis was demonstrated in few observational studies and in small population studies. However, the European Association for the Study of the Liver (EASL), the European Association for the Study of Diabetes (EASD) and the European Association for the Study of Obesity (EASO) recommended the MedDiet for the treatment of NAFLD based on to this moderate-quality evidence in Europe [17]. The MedDiet has been shown to reduce hepatic fat and to improve hepatic insulin sensitivity even without weight loss in patients with NAFLD. Adherence to the MedDiet has also been associated with less advanced NAFLD and low risk of metabolic syndrome in NAFLD patients [74]. The MedDiet also encourages a high-quality lifestyle, including adequate rest periods, physical activity, and sun exposure, which showed positive effect on the NAFLD course [79]. The MedDiet Foundation, in collaboration with the Forum on Mediterranean Food Cultures, has started a process to gather scientific input from international specialists to reach a consensus position on a reviewed description of the MedDiet pyramid [79].
7. Foods and NAFLD Amelioration
The impact of the foods is still controversial due to the limited number of large clinical trials, and the different amounts consumed by the population.
7.1. Nuts
Nuts and seeds are composed of a unique blend of fatty acids and bioactive compounds, such as monounsaturated fatty acids and polyunsaturated fatty acids, vegetable protein, fibre, minerals, vitamins, tocopherols, phytosterols, and polyphenols [80]. All dried fruits have a similar composition in proteins (10–25%), sugars (5–20%), and lipids (50–60%; from 0.51 to 0.73 g/g of fruit), except for chestnuts that are richer in carbohydrates than in fat, and they do not provide cholesterol. Nuts rich in monounsaturated fatty acids, especially oleic acid, are hazelnuts, almonds, and pistachios. Nuts rich in polyunsaturated fatty acids, especially linoleic acid, are walnuts and sunflower seeds. Walnuts are rich in alpha-linolenic acid [80]. Regular consumption of walnuts improves the lipid profile and decreases the incidence of obesity, type 2 diabetes mellitus (T2DM), and hypertension together with MetS. Their consumption is inversely associated with the presence of hepatic transaminases (gamma-glutamyl transferase (GGT), alanine aminotransferase (ALT), and aspartate aminotransferase (AST). Low consumption of nuts and seeds is associated with an increased risk of developing NAFLD in men. A study with 4655 subjects concluded that daily nut consumption is inversely related to advanced fibrosis in NALFD patients [81]. Despite their high energy contents, nut consumption is not associated with weight gain [82]. Nuts improve lipid profile, liver disease, and inflammation, making them useful in a potential treatment for NAFLD [83].
7.2. Extra Virgin Olive Oil (EVOO)
Olive oil contains more than 30 phenolic compounds [84]. It is predominantly comprised of MUFAs (70–80%), such as oleic acid (OA; C18:1 n-9). It has low amounts of linoleic acid ALA (up to 20%) and palmitic acid (up to 20%) [83]. It contains α-tocopherol (5,7,8-trimethyltocol), the most active in vivo form of vitamin E and the most abundant in nature [85]. Extra virgin olive oil (EVOO) is obtained directly from the ripe fruit by physical means (first pressing or centrifugation), and it is the only one that is consumed unrefined [83]. The beneficial effects of EVOO are widely shown. A randomized controlled trial demonstrated that 10 g of EVOO in a MedDiet context decreased postprandial blood glucose levels and low-density lipoprotein LDL and increased insulin level and glucagon-like peptide-1 (GLP-1) [86,87]. In a human study using EVOO as a source of MUFAs to treat patients with T2DM, a reduction in liver fat (39%) was observed [86]. The consumption of EVOO can alleviate the degree of fatty liver in patients treated with a hypocaloric diet [88]. However, the results should be considered as the effect of other components and the hypocaloric diet. A review of EVOO and its liver-protective effects exposed several relevant molecular effects, such as the induction of cellular antioxidant responses, the prevention of inflammatory responses, and the prevention of the endoplasmic reticulum stress, autophagy, and lipogenic responses [89].
7.3. Fish
Omega-3 fatty acids are long chains of polyunsaturated fatty acid (PUFAs). Since fish can synthesize omega-3 fatty acids from ingestion of marine plants [84], omega-3 are mostly found in seafood. Marine omega-3 includes eicosapentaenoic acid (EPA), docosahexaenoic acid (DHA), and docosapentaenoic acid [85]. Deep-water fish (tuna, salmon, mackerel, herring, and sardines, globally called “oily fish”) showed the highest EPA and DHA concentrations, because they store lipids in the flesh, contrary to lean species that store them in the liver (cod) and have lower levels of EPA and DHA [90]. By means of several mechanisms, fish oil omega-3 PUFAs decrease lipid accumulation and hepatic enzyme levels, increase insulin sensitivity, and show anti-inflammatory effects [84,91]. In contrast, thrombotic and inflammatory events, such as cardiovascular disease, cancer, and inflammatory and autoimmune illnesses, are associated with high intakes of omega-6 PUFAs. In the Western diet, an omega-6/omega-3 (proinflammatory: anti-inflammatory) ratio of 15:1 has been reported [92]. Thus, the increase in omega-6/omega-3 is implicated in the development of hepatic steatosis and then NAFLD/NASH [91]. A meta-analysis of the efficacy of omega-3 supplementation in people with NAFLD/NASH during a median duration of 6 months showed that omega-3 polyunsaturated fatty acid supplementation reduced liver fat measured by ultrasound, magnetic resonance imaging, or biopsy and improved liver enzymes (AST and ALT) [88]. The depletion of omega-3 fatty acids is correlated with the development of hepatic steatosis and subsequently NAFLD, NASH, and fibrosis [91]. A study in Japan investigated the dietary intake, abdominal fat, and biochemical data of non-obese and obese NAFLD patients, finding that dietary cholesterol was abundant as well as dietary PUFAs that had lower levels in obese patients and healthy controls, concluding that the altered cholesterol and PUFA intake may be associated with NAFLD in non-obese patients [26].
7.4. Dietary Fibre
Poor fibre consumption may impair NAFLD; however, the exact mechanism is unclear yet [93,94]. Since some fibres are prebiotic, high-fibre diets and whole grains have the potential to influence positively the composition of the gut microbiota, which may be relevant to the hepatic-gut axis in NAFLD progression [95]. The gross intestinal bacteria ferment fibre into short-chain fatty acids, such as butyrate, propionate, and acetate, which delays the progression of NAFLD [96]. Poor fibre intake is common in NAFLD and NASH [92]. The consumption dietary fibres, especially those derived from whole grains, are beneficial to reduce comorbidities associated with MetS and NAFLD. Moreover, to reduce hepatic fat, fibres derived from whole grains may also reduce inflammation [97].
7.5. Legumes
Legumes provide essential nutrients such as vegetable proteins, fibre, minerals, oligosaccharides, phytochemicals, and other bioactive substances such as saponins and polyphenols [98]. There are studies reporting the benefits of legumes. A study among Tehrani adults investigated the relationship between legume intake and a risk of NAFLD and concluded that a high total intake of legumes (beans, lentils, and peas) was significantly associated with a low risk of NAFLD [99]. A significant inverse relationship between legume intake and a risk of cardiovascular disease was also reported in a meta-analysis [100]. Dietary intake of non-soy legumes (lentils, beans, peas, and chickpeas) was associated with high-quality diet, low fat intake, high intake of bioactive compounds and vegetable proteins, small waist circumference, and low serum cholesterol and blood pressure [99,100]. Legumes lowered blood lipids by increasing the excretion of fats and steroids through the faeces and the formation of short-chain fatty acids in the colon [101].
7.6. Fruits and Vegetables
The mechanism underlying the beneficial effects of vegetable and fruit consumption on the NAFLD risk is fully known; however, it has been explained by its reduced energy density after their addition to the diet, as well as the antioxidant activity of polyphenols and carotenoids contents in vegetables and fruits [102]. A cross-sectional study in overweight Latino youth participants concluded that the consumption of non-starchy vegetables was associated with positive metabolic outcomes, including low visceral and liver fat, and increased insulin sensitivity, even when consumed small amounts [103]. A prospective cohort study on a large Korean population sample [102] showed that vegetable and fruit intakes were individually associated with low incidence of NAFLD in women. The total vegetable and fruit intake was related to low incidence of NAFLD in both men and women after a 4.2-year follow-up. A cross-sectional study in Japan showed no significant association between fruit or vegetable intake and NAFLD [104]. It has been pointed out that added fructose, and not natural fructose as being in vegetables and fruits, is the main contributor to the NAFLD development and progression. Fruit and vegetable fructose has no adverse effects on NAFLD, and protects against NAFLD and other related diseases, such as T2DM [105].
7.7. Dairy Products
It has been suggested that dairy products prevent NAFLD due to the contents of whey protein by reducing weight and fat mass [106]. The protective effects of dairy products against NAFLD were attributed to several mechanisms, some connected to insulin resistance. The prevalence of dairy consumption was found to be negatively correlated with the development of the insulin resistance syndrome in the population-based prospective coronary artery risk development in a young adult study [107]. A meta-analysis study revealed that consumption of dairy products, particularly low-fat, had a positive impact on body weight, waist circumference, and the Homeostatic Model Assessment for Insulin Resistance (HOMA-IR) [108]. Cheese and dairy products are a rich source of so-called bioactive peptides [109]. A study conducted in Korea found that high milk protein intake was significantly and inversely associated with the risk of NAFLD incidence in men and women aged ≥50 years. The consumption of milk and other dairy products could prevent the development of NAFLD [110]. A population-based cohort with 7540 adults evaluated the association between the total intake of different dairy products and fatty liver index (FLI), finding a modest inverse correlation between milk consumption and FLI, but they were not able to examine low-fat and high-fat dairy products separately. Nevertheless, they concluded that drinking milk in moderation, especially low-fat varieties (at least one unit more than 5–6 times a week) could ameliorate NAFLD [111]. Yogurt is a food produced by bacterial fermentation of milk, and its consumption delivers many probiotics to the gastrointestinal tract [112]. A cross-sectional study found that high yogurt consumption was associated in a dose-dependent manner with low prevalence of newly diagnosed NAFLD [113]. A randomized double-blinded study demonstrated that the consumption of yogurt containing Lactobacillus acidophilus La5 and Bifidobacterium lactis Bb12 for 8 weeks in patients with NAFLD showed lower liver aminotransferases, total cholesterol, and LDL-cholesterol compared to patients consuming conventional yogurt. Another randomized controlled trial with 102 patients assessed the effects of symbiotic yogurt (containing 108 colony-forming units of Bifidobacterium animalis/mL and 1.5 g inulin) on NAFLD, concluding that symbiotic yogurt consumption improved the hepatic enzyme concentrations [114].
8. Other Foods and Nutrients That Ameliorate NAFLD
8.1. Probiotics
Probiotics are intestinal bacteria or yeast with the ability to confer health benefits on the host [94,115]. The most used bacteria are Bifidobacterium and Lactobacillus strains, which can ameliorate NAFLD [116]. The literature shows that probiotics have therapeutic effects on NAFLD, reducing oxidative and inflammatory liver damage, as well as lowering hepatic triglycerides (TG) and hepatic steatosis [117,118]. Altered gut microbiota is associated with obesity, a risk factor for NAFLD. An increase in the strain Firmicutes and a decrease in Bacteroidetes were described in obesity [119]. Prebiotics are nutrients used by host microorganisms, and they can modulate the composition of the gut microbiota involved in NAFLD development. In Asian NAFLD patients (n = 75) using probiotics and prebiotics, there was a decrease in body weight and amelioration of NAFLD parameters [120]. A review highlighted that NASH patients treated with Lactobacilli strains plus Bifidobacterium bifidum showed low triglyceride liver contents measured by magnetic resonance imaging, but these effects in NASH should be further tested in larger studies [24].
8.2. Coffee
Coffee protects against the NAFLD development and decreases the NASH severity. The unsweetened filtered coffee could be a reasonable adjunct to diet and exercise in patients with fatty liver [121]. Coffee contains caffeine, phenols, chlorogenic acids, sugars, organic acids, polysaccharides, and aromatics, among more than thousand compounds. Two decades ago, the protective effect of coffee consumption against cirrhosis was reported [122]. A growing body of evidence suggested the beneficial effects of coffee on NAFLD by means of both a direct effect on the liver and systemic metabolic effects. Lately, a high reduction in the risk of T2DM and cardiovascular disease was demonstrated in coffee drinkers [123,124]. The US National Health and Nutrition Examination Survey 2001–2008 showed that caffeine and plain water intakes were independently related to a low risk of NAFLD, regardless of race, gender, clinical parameters, metabolic syndrome components, and dietary constituents [125]. Patients with NAFLD/NASH showed a reduced risk of liver fibrosis after taking coffee. Two meta-analyses concluded that coffee consumption was associated with a 29% lower risk of NAFLD, 30–39% lower risk of liver fibrosis, and a 39% lower risk of cirrhosis; however, the limitation was the definition of regular coffee consumption, because it changed between studies [126]. One study also assessed regular consumption of filtered coffee, but not espresso, and found that it was independently associated with low fibrosis [127]. It was pointed out that espresso drinkers usually added sugar, which explains the benefits of filtered coffee. Caffeine is perhaps the coffee’s best-known compound [127]. Coffee can protect the liver by increasing PPAR-α-mediated fatty acid oxidation, decreasing collagen deposition, and promoting an overall increase in protective antioxidants [128]. Chlorogenic acid, caffeine, and kahweol exhibit antifibrotic properties by the inhibition of hepatic stellate cell activation via the downregulation of the transforming-growth-factor-β (TGF-β) pathway and by inhibiting the connective-tissue growth factor [129,130]. Regarding the dosage of coffee consumption, a meta-analysis described a nonlinear relationship between a reduced risk of NAFLD and consumption of >3 cups/d [131]. A cross-sectional study, where coffee consumption was assessed for 6 months, showed low odds of liver fibrosis after a daily consumption of >2 cups [132]. Low fibrosis score was shown in people that drank more coffee (>3/day); thus, coffee intake can have beneficial effects on fibrosis progression [133].
Coffee consumption may also reduce the risk of developing hepatocellular carcinoma. Consumers of ≥3 cups/day showed a 44% lower risk of developing hepatocellular carcinoma [134]. High levels of coffee consumption were related to a lower risk of incident hepatocellular carcinoma (HCC) and chronic liver disease (CLD) mortality compared to non-coffee drinkers; the benefits were observed in those who drank 2–3 cups per day, and the benefits were higher for those who drank ≥4 cups per day. Moreover, the inverse associations were similar regardless of the participants’ ethnicity, sex, body mass index, smoking status, alcohol intake, or diabetes status [135]. Interestingly, the benefits of coffee consumption could be extended to the gut microbiota, as the literature reported possible associations such as an increase in Bifidobacterium spp. [136,137] and a decrease in Escherichia coli and Clostridium spp. [137]. Coffee consumption is associated with microbial richness in patients with cirrhosis [115,138].
8.3. Choline
Choline is an essential group B vitamin obtained from both dietary intake (egg yolks and animal protein) and endogenous synthesis, which is mainly metabolized and stored in the liver [139]. Choline is an essential nutrient, and the central organ responsible for choline metabolism is the liver; hepatosteatosis and death of hepatocytes occur when humans are deprived of choline [140]. In humans, choline deficiency affects NAFLD by inducing irregular phospholipid synthesis, defects in lipoprotein secretion, oxidative damage due to mitochondrial dysfunction, and endoplasmic reticulum stress. The requirement of choline to prevent liver dysfunction is dependent on genetic variations and oestrogen status [140]. Human choline requirements are highly individualized, and biomarkers of choline status are useful to predict the risk of NAFLD [140].
8.4. Micronutrients
Micronutrients are necessary for enzyme function, intermediate metabolism, and the metabolic response to sickness. They include electrolytes, minerals, vitamins, and carotenoids [141]. The excess or lack of micronutrients might exacerbate tissue injury and perturbations of energy homeostasis in NAFLD patients by disrupting the lipid homeostasis and antioxidant pathways. It was suggested that understanding the involvement of micronutrients in NAFLD may help to better understand non-obese NAFLD [142]. The relevant micronutrients involved in NAFLD are zinc, copper, iron, selenium, magnesium, vitamins A, C, D, and E, and carotenoids with the antioxidant, antifibrotic, immunomodulatory, and lipo-protective effects proposed as the mechanisms of the impact of micronutrients on NAFLD [142]. Zinc and copper deficiencies were observed in NAFLD [143,144]. Zinc supplementation showed favourable effects on glycaemic parameters and plasma lipids [145]. However, an excess of iron and selenium may increase the severity of NAFLD [142]. Hepatic iron accumulation in reticule-endothelial cells occurs in NAFLD, and it is associated with the NAFLD pathogenesis, but data are often conflicting [146,147]. Vitamin A, B3, B12, C, D, and E deficiencies—mostly of a low severity—were linked to NAFLD. Vitamin E is an important antioxidant which was used as treatment, decreasing transaminase levels and liver lobular inflammation, improving liver fibrosis, and reducing steatosis [148]. Vitamin E supplementation is a usual practice in NAFLD patients to diminish high oxidative stress. Nevertheless, vitamin E supplementation could have side effects, including an increase in the risk of several kinds of cancer or haemorrhagic stroke, which are the key factors in reducing its use in the clinical practice [25]. Vitamin D protects against the NAFLD and cardiovascular disease by improving insulin sensitivity, reducing inflammation of the adipose tissue, reducing liver inflammation and fibrosis [149]. Low serum vitamin D levels may result in NAFLD, and the severity and incidence of NAFLD are linked to hypovitaminosis D [150]. A recent study in Chinese population showed that low serum vitamin D level was associated with NAFLD in obese but not lean participants [151]. Carotenoids can be found in abundance in colourful fruits and vegetables, and carotenoid-rich foods may be more effective in preventing NAFLD than those with low carotenoid levels [152].
8.5. NAFLD, Oxidative Stress, Inflammation, and Mediterranean Diet
Disturbances in lipid metabolism led to liver lipid accumulation, affecting reactive oxygen species (ROS) genesis. Oxidative stress and inflammation play an important role in the development of chronic diseases, such as NAFLD, and then they could be crucial targets in dietary strategies for disease prevention. It was demonstrated that the severity of NAFLD is related to an increase in oxidative stress and proinflammatory status. Plasma levels of catalase, irisin, interleukin-6, malondialdehyde, and cytokeratin 18 were higher in subjects with more than 17.4% of intrahepatic fat contents measured by magnetic resonance imaging, whereas the resolvin D1 levels were lower [153].
There is evidence that plant-based dietary patterns, such as MedDiet, are associated with low oxidative stress and inflammation, providing useful ways for chronic disease prevention [154].
A one-year nutritional intervention (with hypocaloric Mediterranean diet) improved the main NAFLD features in 40–60-year-old patients, decreasing body mass index, intrahepatic fat contents, glycosylated haemoglobin, markers of liver damage (ALT, AST, GGT, and cytokeratin-18), and prooxidant (malondialdehyde, myeloperoxidase, zonulin, and omentin) and proinflammatory status (decrease in dietary inflammatory index, C reactive protein, ectodysplasin-A, interleukin-1ra, and interleukin-6) and improving the antioxidant (catalase plasma levels and gene expression in peripheral blood mononuclear cells) and anti-inflammatory (irisin and resolvin D1) effects. There was also a decrease in the concentration of plasmatic endotoxin, suggesting an improvement in intestinal permeability [155,156,157,158].
Evidence highlighted the role of two-series prostaglandins in NAFLD pathogenesis, decreasing insulin secretion and pancreatic β-cell proliferation, increasing gluconeogenesis, enhancing hepatic lipogenesis, and decreasing triglyceride output, thus establishing negative effects on liver inflammation and NAFLD progression [159].
NADPH oxydase (NOX) enzyme isoforms exert both metabolism and inflammation regulatory effects, decreasing liver fibrosis, triglycerides production, inflammation, steatosis, insulin resistance, and ROS generation and increasing insulin resistance [160]. However, these effects were demonstrated in mice and cellular models, and they need to be proved in humans.
In addition, 8-iso-prostaglandin F2α was related to some acute-phase-reactant proteins, providing a biochemical link between lipid peroxidation, inflammation, and genesis of NAFLD and other chronic diseases [161]. Therefore, it can be considered as a useful biomarker of oxidative stress in T2DM and related comorbidities, such as NAFLD [162]. Polyphenols contained in the diet, such as MedDiet, produce changes in biomarkers related to the oxidant/inflammatory status, such as 8-iso-prostaglandin F2α [163].
Healthy diet, physical activity, prebiotics, probiotics, and healthy faecal microbiota transplantation are the new therapeutics to prevent hepatic oxidative stress in the future [164].
9. Conclusions
A high-quality diet could improve liver steatosis. Mediterranean diet together with physical activity and limited sugar intake is a good strategy for managing NAFLD. Specific dietary recommendations are added in this manuscript, and a Mediterranean plate is proposed to ameliorate NAFLD (Figure 1 and Figure 2).
Drinking 100 percent fruit may juice sound like a healthy option, but it’s a far cry from eating the real deal—whole, fresh fruit. The sugar is fruit is
In fact, new research finds that drinking just one glass of 100 percent fruit juice every day leads to gaining close to half a pound over three years. Yet increasing whole fruit intake by one serving each day resulted in about a pound of weight loss over three years.
Why is eating whole fruit better for you than drinking juice? Here’s a look at how fruit juice affects your body and how it’s different from eating whole fruit.
The Sugar Problem
A single six-ounce serving of 100 percent fruit juice contains:
About 15 to 30 grams of sugar
60 to 120 calories
What’s more, fruit juice has truly little fiber—even pulp in orange juice doesn’t provide much of the nutrient. The high sugar and low fiber content of juice means that it can spike blood sugar levels and increase your appetite. Over time, this combination can lead to weight gain.
In the study of nearly 50,000 postmenopausal women, researchers found that weight gain among fruit juice drinkers was on par with those who regularly consumed sugary drinks like soda.
THE Whole Fruit IS BEST
Whole, fresh fruit is full of fiber. Fiber-rich fruits can help you feel full while eating fewer calories. Dietary fiber in fruits can also help reduce cholesterol and may lower the risk for heart disease.
Here are some ideas to add more fruit into your diet:
Mix them into your salads.
Snack on dried fruit like raisins, dates, or apricots.
Add sliced apple or banana to your peanut butter sandwiches.
Sprinkle fruit, such as berries, into your pancake or waffle batter.
High-fructose corn syrup is a liquid sweetener made from corn. When corn starch is broken down into individual molecules, it becomes corn syrup, which is 100% glucose, a simple sugar. Enzymes are added to convert some of this glucose into fructose.
High-fructose corn syrup was introduced in the 1970s. It has the same calories as other added sugars. High-fructose corn syrup is cheaper than sugar, with better flavor enhancement and longer shelf life. It’s more stable and consistent, especially in acidic foods and drinks.
As a result, high-fructose corn syrup went from 1% of sweeteners in the U.S. in the 1970s to 42% by 2004. From 1977 to 1978, the average American consumed about 37 grams of fructose per day. In 2008, this jumped to 54.7 grams, about 10.2% of total daily calories. The number was even higher in teenagers, at 72.8 grams per day.
Americans get fructose mostly in sweetened drinks (30%), grains (22%), and fruit or fruit juice (19%).
Foods with high-fructose corn syrup include:
Fast food items
Breakfast cereals
Bread and baked goods
Sweetened dairy products like yogurts
Candies
Canned foods like soups and fruit
Soft drinks
Is High-Fructose Corn Syrup Bad For You?
High-fructose corn syrup isn’t all that different from sugar. The two most common forms contain either 42% or 55% fructose, as well as glucose and water. Regular sugar is 50% fructose and 50% glucose.
Obesity. Many things affect your obesity risk — such as physical activity, stress, and your genes — but getting an excessive amount of sugar may play a role. It’s possible that fructose doesn’t stimulate the parts of the brain that control appetite. However, more studies are needed.
Liver problems. Getting too much fructose can raise your risk of nonalcoholic fatty liver disease. This is when too many fats are stored in liver cells. When you have too much fat buildup, it can lead to nonalcoholic steatohepatitis, scarring of the liver, and liver damage and cirrhosis
High triglycerides. Studies have shown that fructose can raise triglycerides in the blood. Triglycerides contribute to health issues like arteriosclerosis (the thickening of the artery walls) and pancreatitis (inflammation of the pancreas). Researchers found that a 6-week diet of 17% fructose led to a 32% increase in triglycerides.
More uric acid. Fructose can also stimulate uric acid production. Too much uric acid can lead to gout, a painful type of arthritis.
Type 2 diabetes.Insulin is a hormone that your pancreas makes to regulate blood sugar. If you have type 2 diabetes, it means your body can’t use insulin the way it should. In a small study in which healthy adults drank sweetened drinks for 3 weeks, scientists found that even moderate amounts of fructose and sucrose changed how responsive their cells were to insulin.
How to Cut Down on High-Fructose Corn Syrup
Read ingredient labels. It may be in more processed foods than you think.
Cut down on sodas and other sweetened drinks. Drink water instead. Add berries, lemon, lime, or cucumber if you need more flavor.
Snack on whole foods like nuts and fruits instead of cookies and candy.
Go with homemade baked goods instead of store-bought ones.